Downloaded 540 times
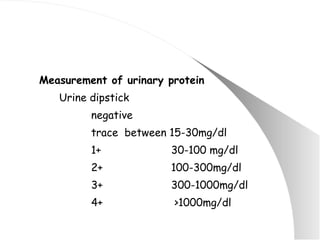
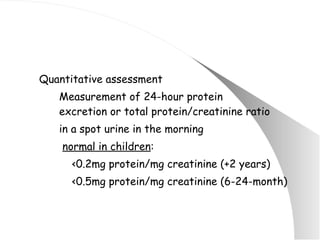

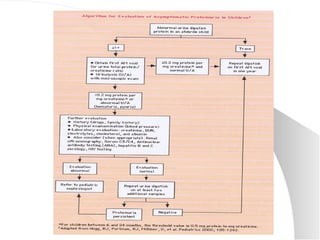
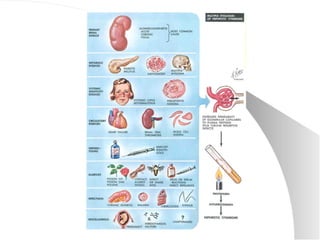

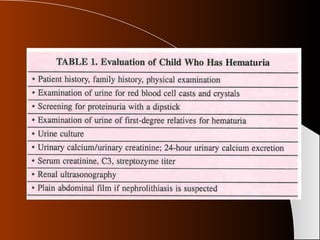


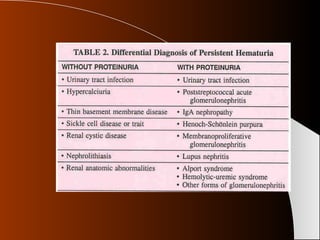
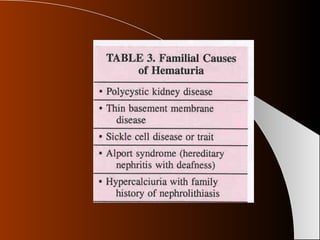
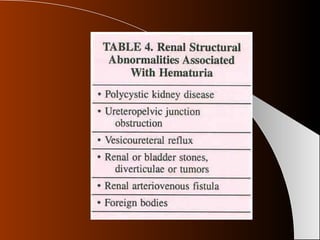

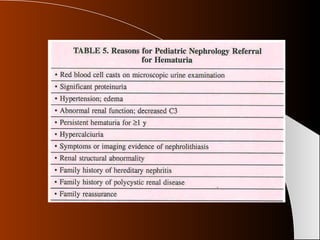

The document discusses proteinuria and hematuria in children. It covers the definition, causes, evaluation, and treatment of both conditions. Proteinuria can be caused by glomerular, tubular, or overflow mechanisms and is evaluated through urine dipsticks, 24-hour urine collection, and urine protein to creatinine ratio. Hematuria can be gross or microscopic and is seen in conditions like UTI, nephrolithiasis, glomerulonephritis, IgA nephropathy, and Alport syndrome. Evaluation of hematuria involves urinalysis, urine culture, imaging, and considering familial causes. Specific renal diseases like post-streptococcal glomerulonephritis



































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





