
Download to read offline

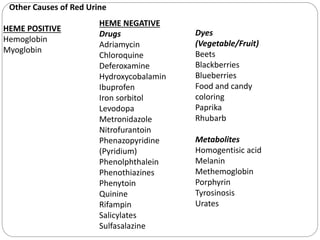
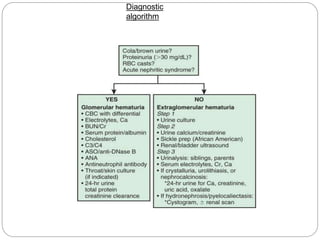
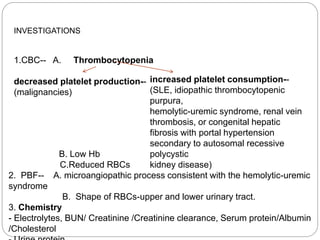
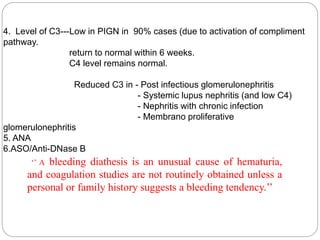
This document provides an overview of hematuria in children, including definitions, causes, evaluation, and diagnostic approach. It begins by defining hematuria and discussing qualitative urine dipstick tests. Potential causes of hematuria are then outlined, separated into upper and lower urinary tract sources as well as isolated renal, multisystem, tubulointerstitial, and anatomic disorders. Evaluation involves history, exam, urinalysis to determine hematuria level and urgency. Further tests may include CBC, chemistry, coagulation studies, C3 level, ANA, cystoscopy. Children with isolated microscopic hematuria and normal evaluation should be monitored every 3 months until resolved. Renal biopsy is indicated for persistent hematuria with other abnormalities.





















































