Downloaded 85 times



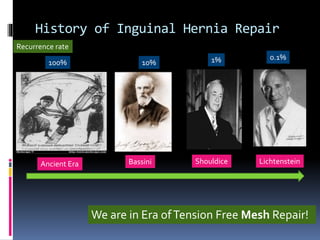


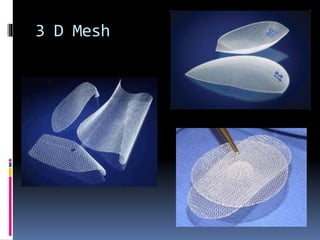

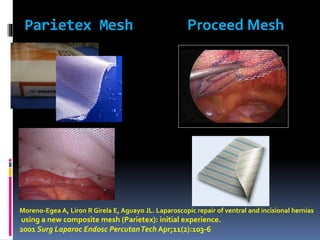
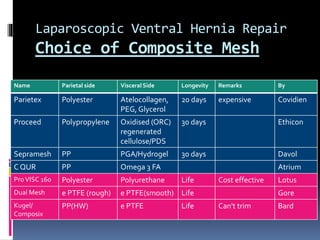
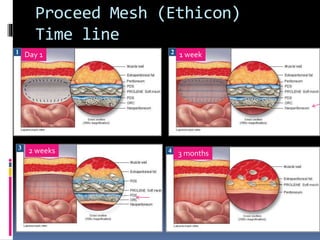
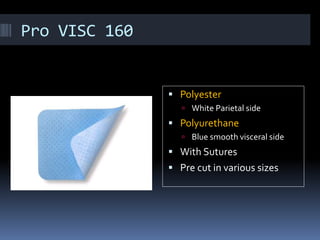
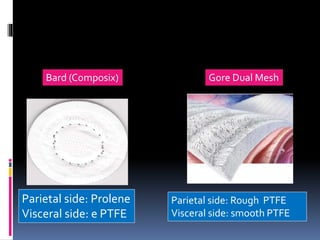
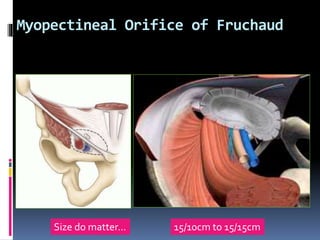
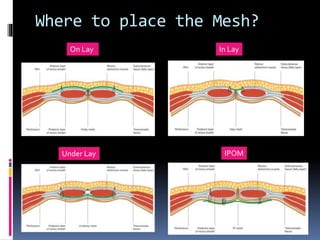
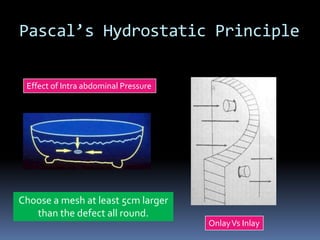
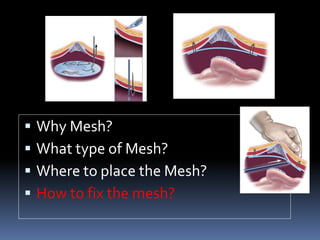

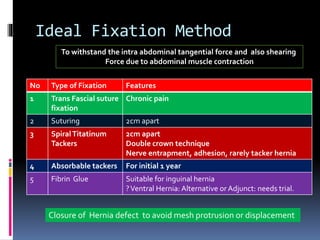


The document discusses abdominal wall hernia repair using prosthetic materials and fixation devices. It notes that mesh repair has become the standard of care due to its low recurrence rates when done tension-free. Different types of meshes are described including synthetic, absorbable, composite and biological meshes. Placement techniques including onlay, inlay and IPOM are covered. Fixation methods such as tacks, staples, sutures and fibrin glue are also discussed. The document emphasizes that composite meshes are preferred for ventral hernia repair and that secure fixation is important to prevent recurrence.





























































































