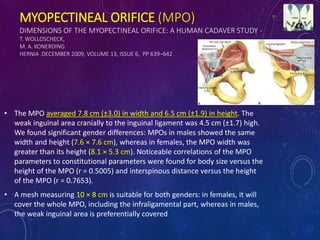
The document discusses various aspects of meshes used in laparoscopic hernia surgery, detailing types such as tension-free and tension repairs, along with the characteristics of the myopectineal orifice. It highlights the differences in mesh types, including lightweight and partially absorbable meshes, and their respective impacts on postoperative outcomes such as chronic pain and recurrence rates. Additionally, it addresses the methods of mesh fixation and offers guidelines on mesh selection based on the type of hernia and patient considerations.