Downloaded 953 times
















![Am J Surg. 2009 Jan;197(1):64-72. Epub 2008 Jul 9.Laparoscopic versus open repair of incisional/ventral hernia: a meta-analysis.Sajid MS, Bokhari SA, Mallick AS, Cheek E, Baig MK.: Am J Surg . 2009 Sep;198(3):463. BACKGROUND : The aim of this article is to analyze laparoscopic versus open repair of incisional/ventral hernia (IVH). METHODS: A systematic review of the literature was undertaken to analyze clinical trials on IVH. RESULTS: Five randomized controlled trials involving a total of 366 patients were analyzed. There were 183 patients in each group. Open repair of IVH was associated with significantly higher complication rates and longer hospital stays than laparoscopic repair. There was also some evidence that surgical times may be longer for open repair of IVH. However, statistically there was no difference in wound pain or recurrence rates. CONCLUSIONS: Laparoscopic repair of IVH is safe, with fewer complications and shorter hospital stays, and possibly a shorter surgical time . However, postoperative pain and recurrence rates are similar for both techniques. Hence, the laparoscopic approach may be considered for IVH repair if technically feasible, but more trials with longer follow-up evaluations are required to strengthen the evidence.PMID: 18614144 [PubMed - indexed for MEDLINE]](https://image.slidesharecdn.com/ventralherniachallengesandchoices-110210093435-phpapp01/85/Ventral-Hernia-Challenges-and-Choices-115-320.jpg)

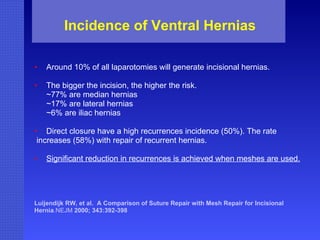
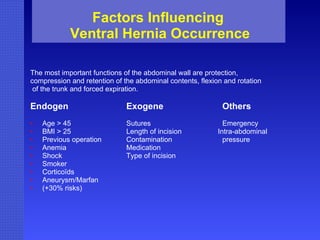
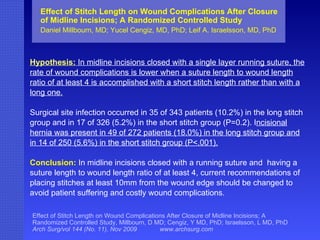
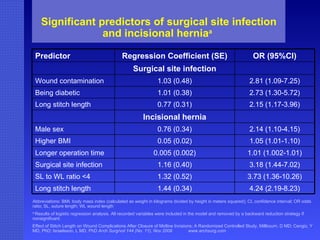
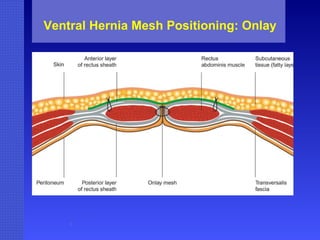
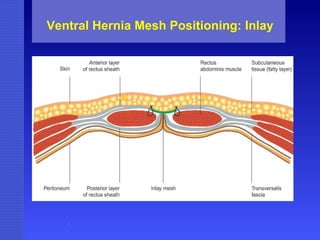
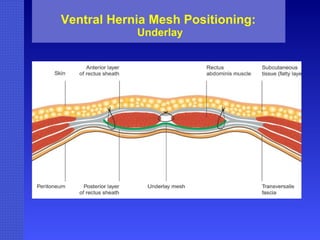
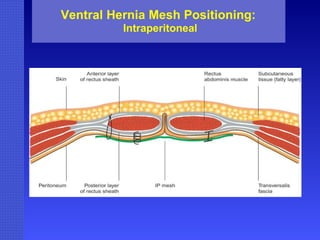
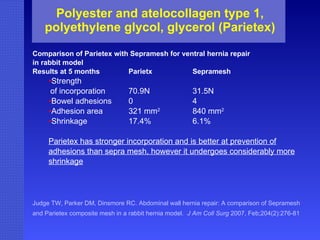
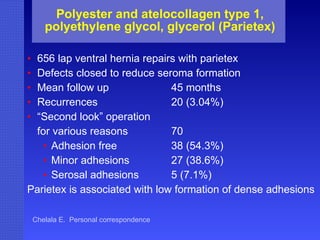
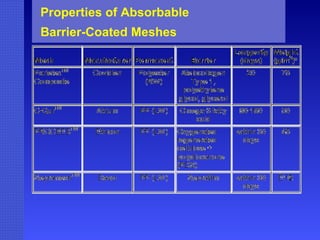
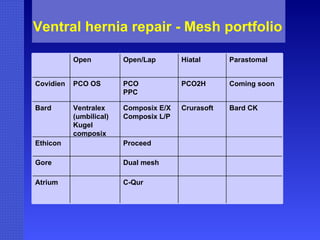
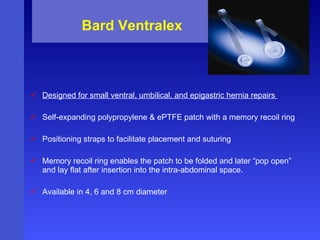
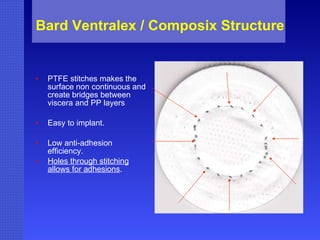
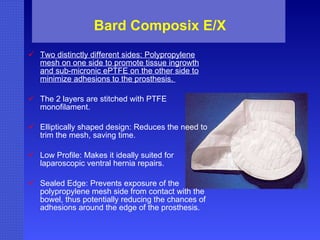
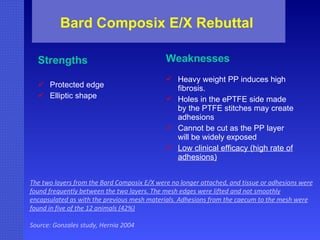
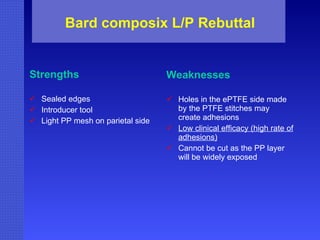
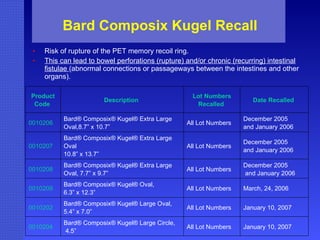
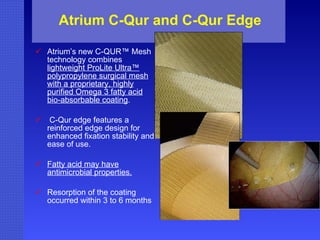
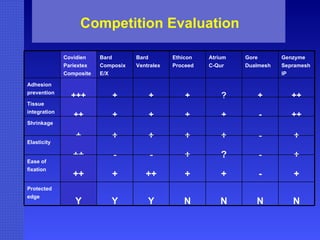
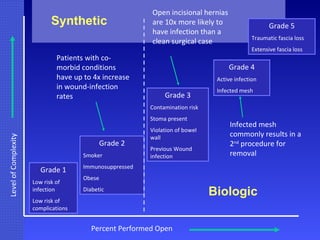
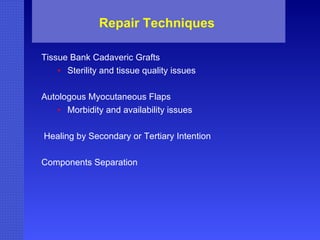
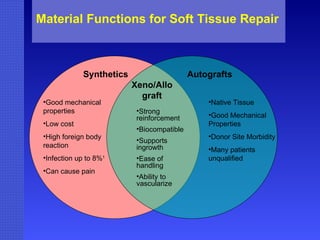
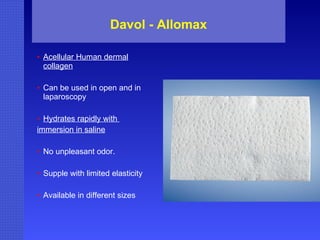
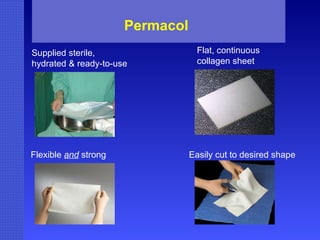
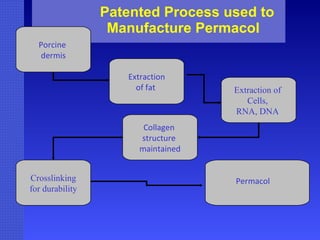
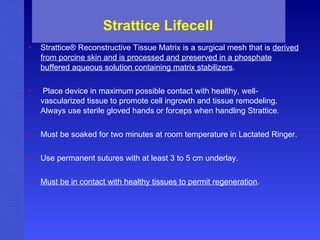
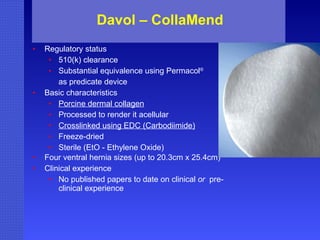
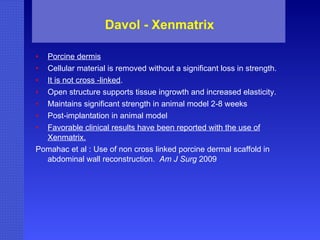
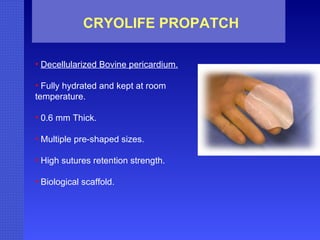
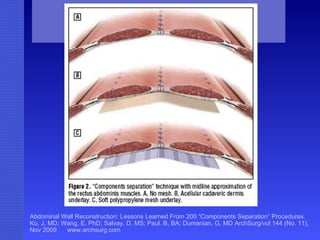
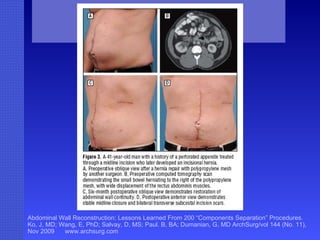
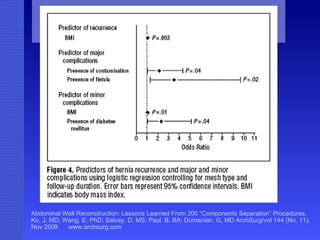
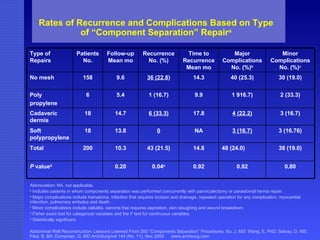
The document discusses ventral hernias, including: - Incidence and risk factors for ventral hernias - Options for mesh placement during hernia repair surgery - Types of prosthetic meshes used, including benefits and disadvantages of polypropylene, ePTFE, polyester, and absorbable barrier-coated meshes - Studies comparing surgical outcomes and complications between different mesh types







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















