Downloaded 360 times
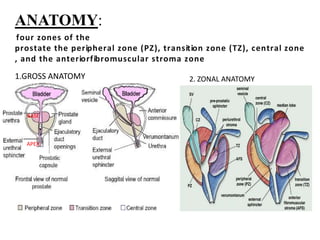
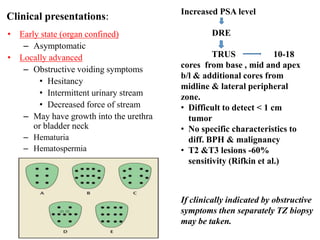
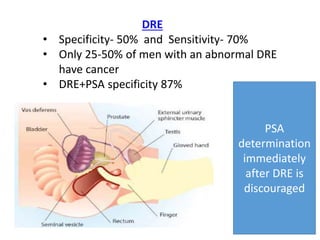
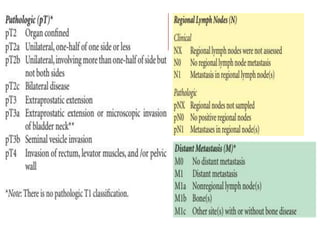
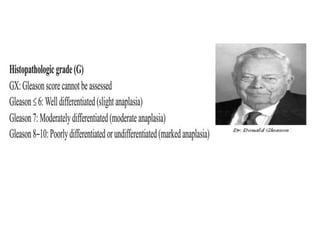
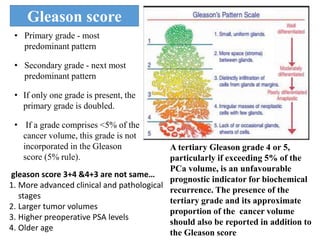
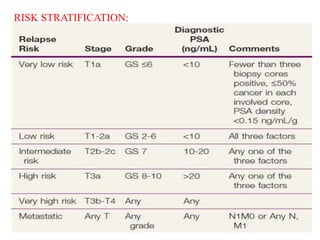
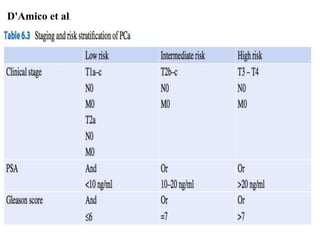


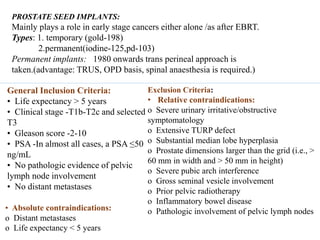
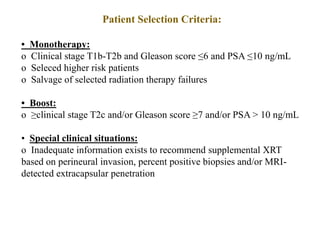
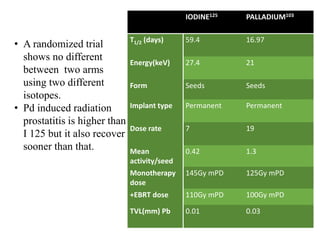

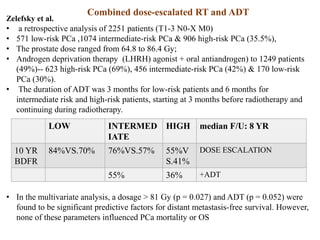
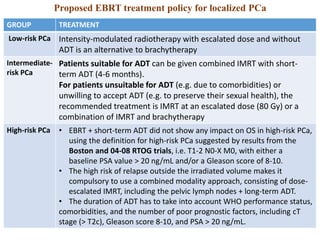
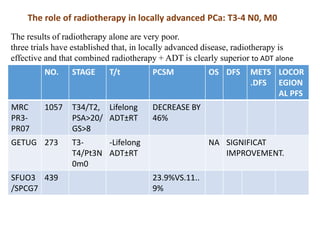
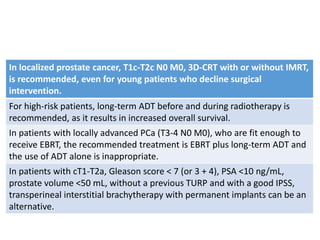
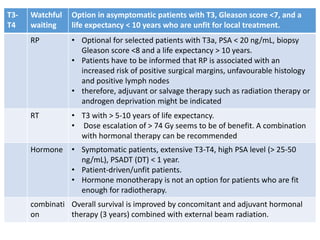
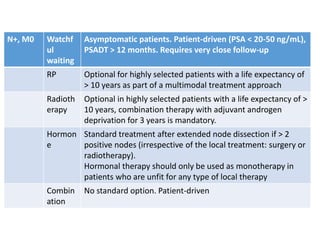
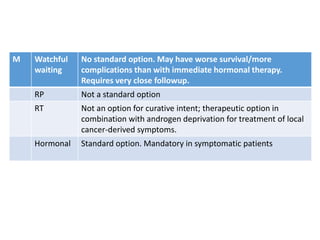

The prostate is a gland that produces seminal fluid. Prostate cancer is the second most common cancer in men. The prostate has four zones - peripheral, transition, central and anterior fibromuscular. Prostate cancer usually arises in the peripheral zone and is typically an adenocarcinoma. Diagnosis involves a digital rectal exam, prostate-specific antigen testing, transrectal ultrasound of the prostate and biopsy. Staging involves evaluating if the cancer is organ-confined or has spread locally or metastasized. Treatment options depend on risk stratification and may include active surveillance, surgery, radiation therapy or hormone therapy.








































![Ca prostate [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/caprostateedmond-130318091345-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

























