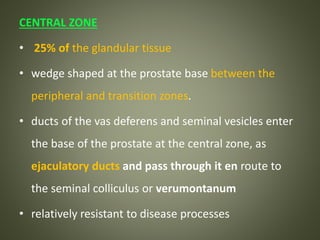
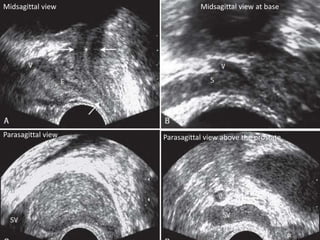
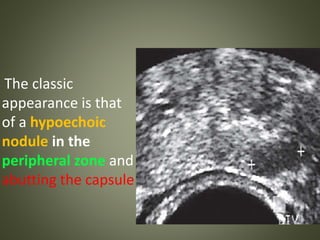
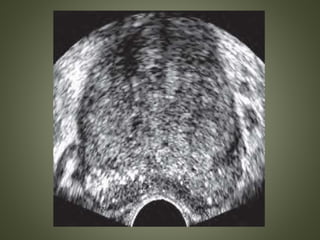
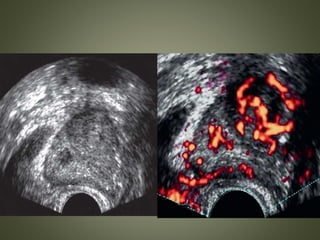
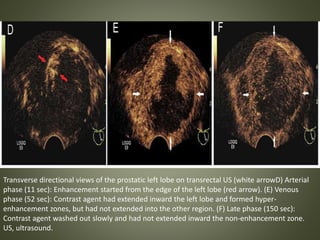
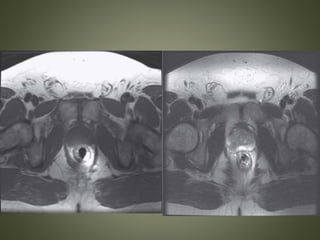
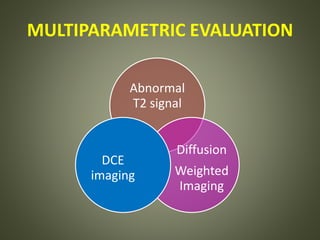
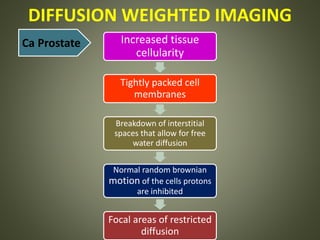
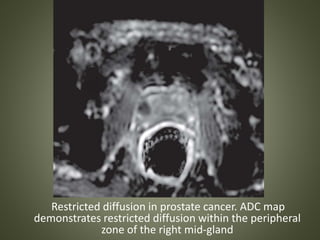
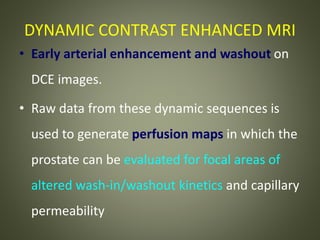
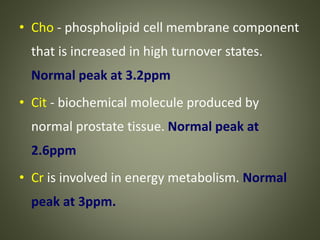
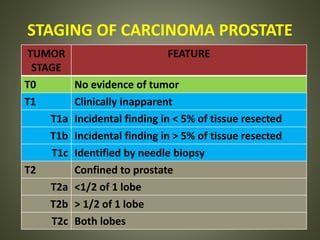
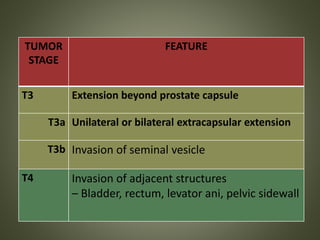
Prostate carcinoma is the most common malignancy in males, typically affecting men over 50 years old. On transrectal ultrasound (TRUS), prostate carcinoma usually appears as a hypoechoic lesion in the peripheral zone. Multiparametric MRI with T2-weighted, diffusion-weighted, and dynamic contrast-enhanced sequences is the most sensitive imaging method for detecting prostate carcinoma, as it can identify restricted diffusion and abnormal enhancement patterns not seen on ultrasound. While imaging is useful for detection and staging of prostate carcinoma, biopsy remains the standard for diagnosis.









![PROTOCOL ADVICE
– High-resolution T2WI +
□ DWI
□ Dynamic contrast-enhanced MR (DCE-MR)
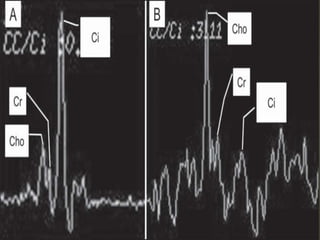
□ MR spectroscopy (MRS [optional])
– Pelvic phased array coil + endorectal coil
– 1.5T-3.0T MRI
– > 6 weeks post biopsy](https://image.slidesharecdn.com/prostatecarcinoma-171215141938/85/Prostate-carcinoma-81-320.jpg)




















































![Spleen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/spleen1-171112094140-thumbnail.jpg?width=640&height=640&fit=bounds)


![Radiological anatomy of_abdomen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyofabdomen1-170830125353-thumbnail.jpg?width=640&height=640&fit=bounds)

![Stomach and duodenum_-_benign_lesions[2]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenum-benignlesions2-171112093735-thumbnail.jpg?width=640&height=640&fit=bounds)

![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)




















