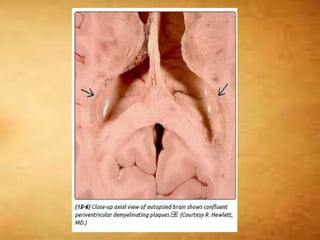
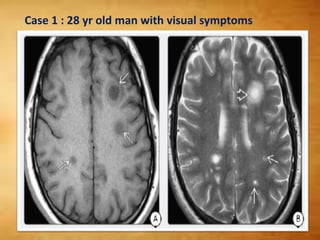
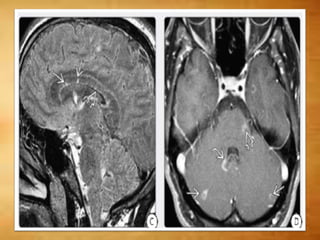
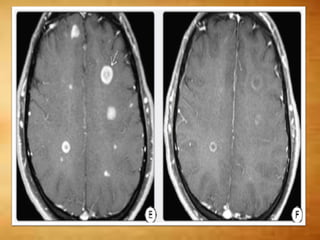
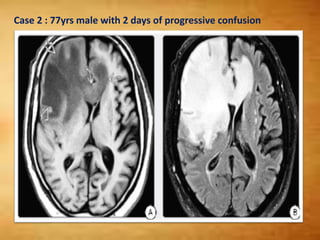
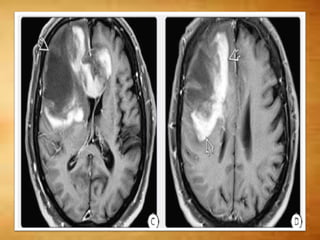
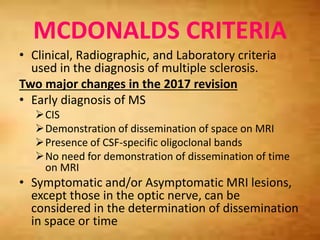
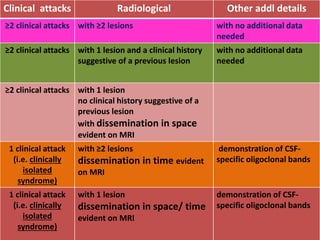
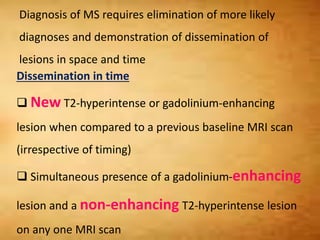
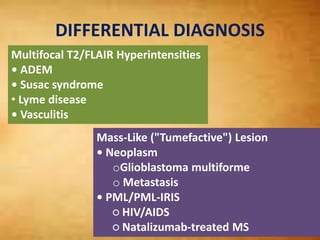
This document summarizes multiple sclerosis (MS), a chronic inflammatory demyelinating disease of the central nervous system. It discusses the etiology, pathology, clinical presentation, imaging features, diagnostic criteria, variants, and differential diagnosis of MS. Key points include: MS is characterized by inflammatory demyelinating lesions ("plaques") in the brain and spinal cord; risk factors include genetic and environmental factors; clinical presentation varies from relapsing-remitting to progressive forms; MRI is important for diagnosis and demonstrates disseminated hyperintense lesions; and differential diagnosis includes ADEM, Susac syndrome, and CNS tumors.
























































![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)
![Spleen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/spleen1-171112094140-thumbnail.jpg?width=640&height=640&fit=bounds)
![Stomach and duodenum_-_benign_lesions[2]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenum-benignlesions2-171112093735-thumbnail.jpg?width=640&height=640&fit=bounds)

![Radiological anatomy of_abdomen[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyofabdomen1-170830125353-thumbnail.jpg?width=640&height=640&fit=bounds)



















