Downloaded 75 times




![Talking with Patients – Value of
In primary care,
about 86% of the
Diagnostic value is
from historical data
[ Ref - Hampton JR et al.
BMJ 1975;2: 486-9]
History
Exam Lab](https://image.slidesharecdn.com/4003b361-f067-4fc4-b946-aebd89dfbc75-150719172246-lva1-app6892/85/Clinical-Skills-Training-and-Simulation-Pedagogy-33-320.jpg)
![Learning to Elicit
History
• Role play simulation!
• Let them play Doctor-
Patient roles and learn
“There is no cement like interest;
no stimulus like the hint of
practical consideration." [A Flexner-1910]](https://image.slidesharecdn.com/4003b361-f067-4fc4-b946-aebd89dfbc75-150719172246-lva1-app6892/85/Clinical-Skills-Training-and-Simulation-Pedagogy-34-320.jpg)


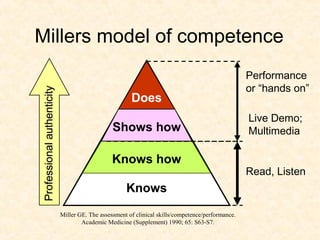
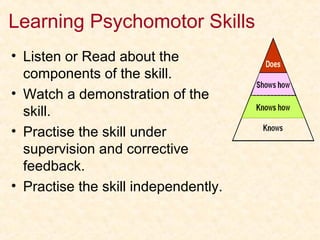
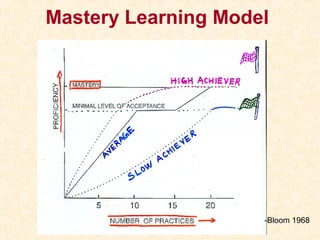
This document discusses clinical skills training and simulation pedagogy. It outlines various objectives of the session which include listing competencies for health professionals, discussing taxonomy of skills and methods for learning them using Dale's Cone model. It also explains simulation pedagogy using Miller's Pyramid of competence and discusses advantages of using simulation as a teaching tool, including how debriefing and reflection are important parts of simulation-based education. The document provides examples of skills that can be taught via simulation and examines research on implementing simulation effectively in learning.




































































































