Downloaded 15 times





















This document discusses common oral health problems and their causes and treatments. It covers dental plaque, calculus, gingivitis, periodontitis, dental caries, hypersensitivity, staining, malodor, dry mouth, ulcers, and types of oral preparations like toothpastes and mouthwashes. Dental plaque builds up and leads to calculus formation, which can cause gum disease. Tooth decay occurs when acids from plaque dissolve tooth enamel. Periodontitis is a serious gum infection causing bone loss. Various formulations are provided as examples to address issues like cavities, plaque, sensitivity, and breath freshening.
Introduces common oral problems affecting health and aesthetics, including medical issues like caries and cosmetic issues like staining.
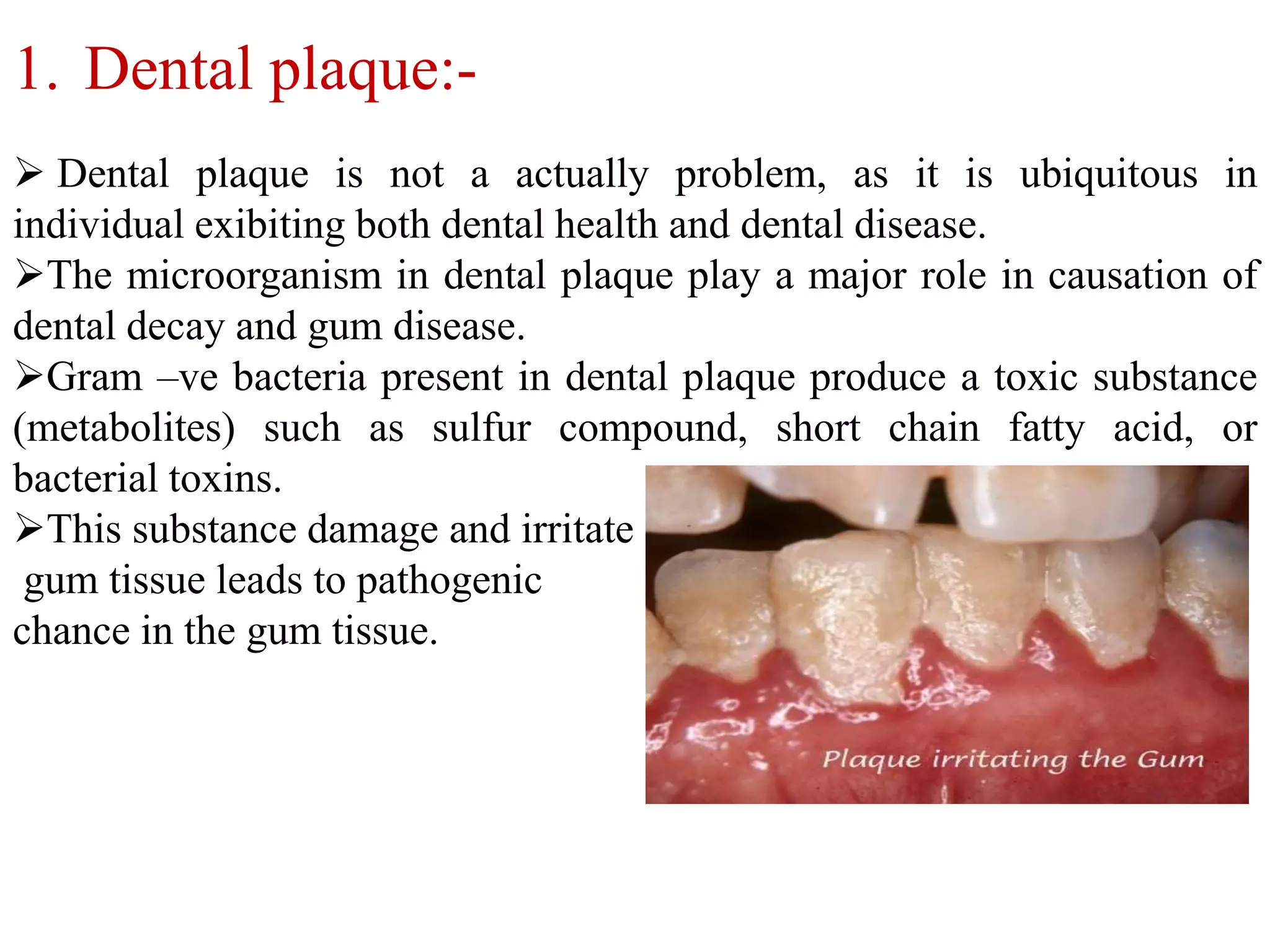
Discusses dental plaque's role in oral health and disease; explains calculus formation and its effects.
Covers gingivitis and periodontitis; highlights their causes, symptoms, and treatment options.
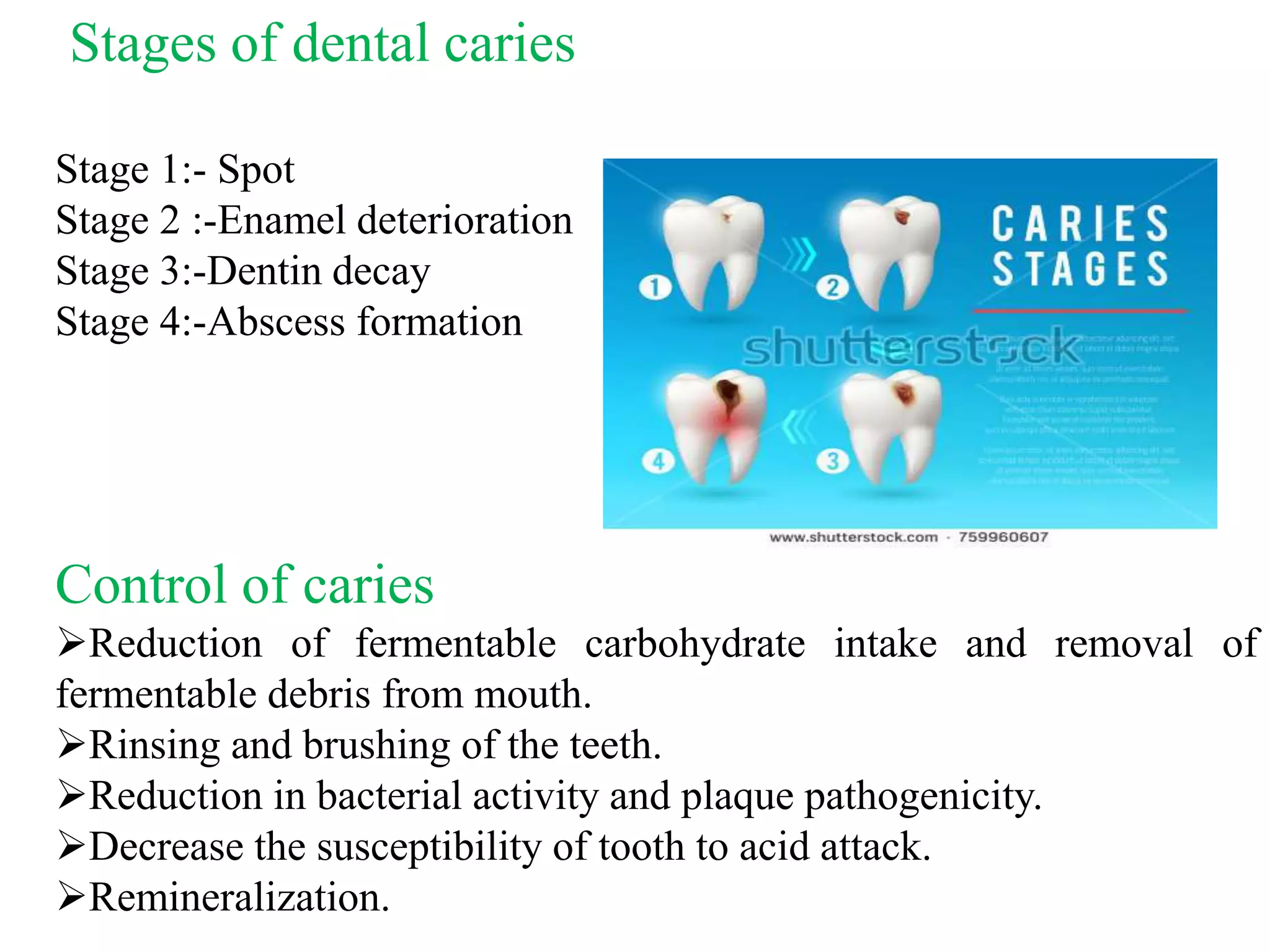
Explains tooth decay, its stages, causes, and management strategies like diet control and oral hygiene.
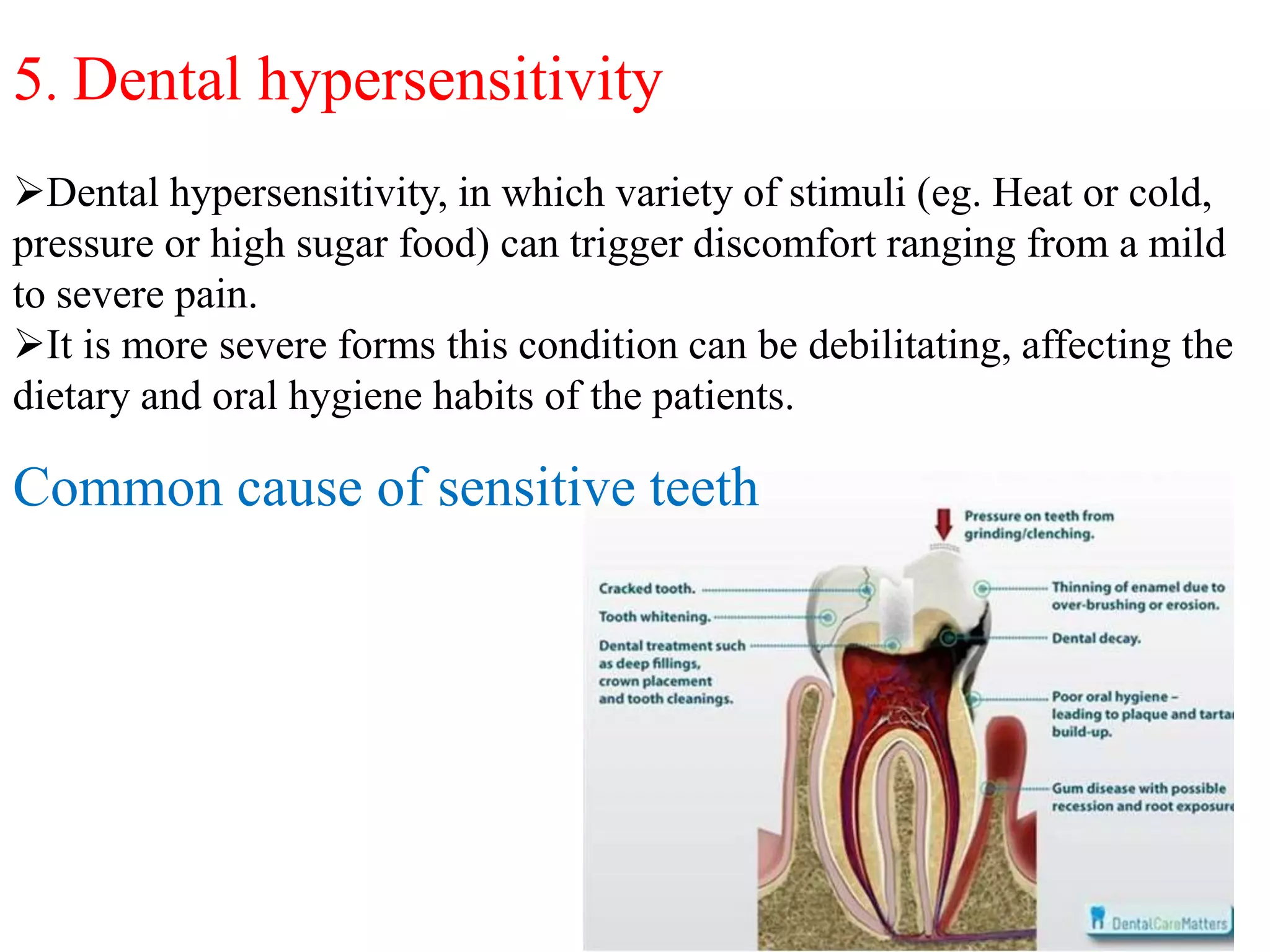
Describes triggers of dental sensitivity and underlying mechanisms, along with management approaches.
Categorizes intrinsic and extrinsic dental staining, treatment options for discoloration.
Explains xerostomia causes including medications and effects; describes management strategies.
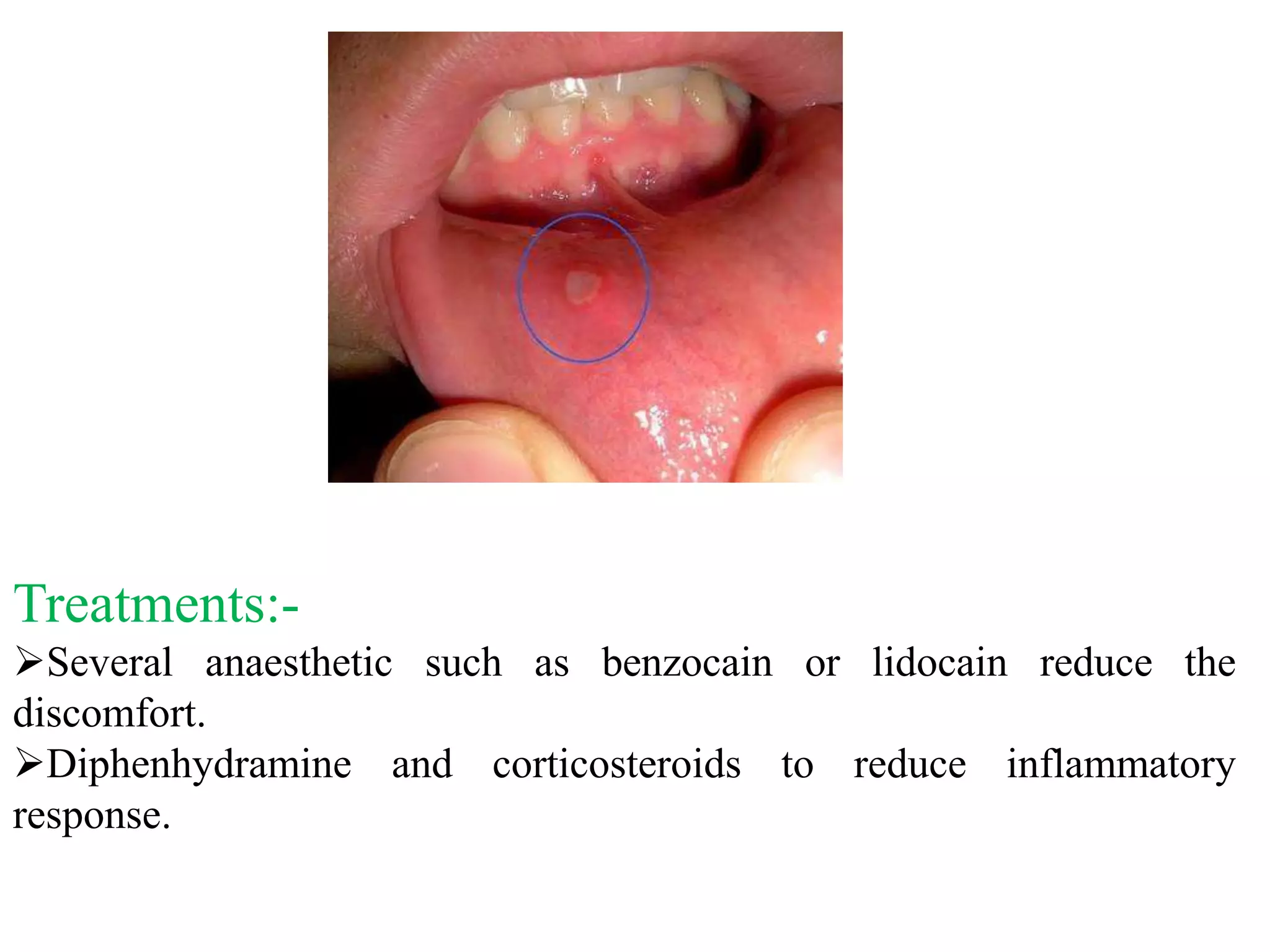
Defines canker sores, causes, and treatments including mouth rinses and pain relief options.
Introduces various dental products like dentifrices aimed at maintaining oral hygiene and health.
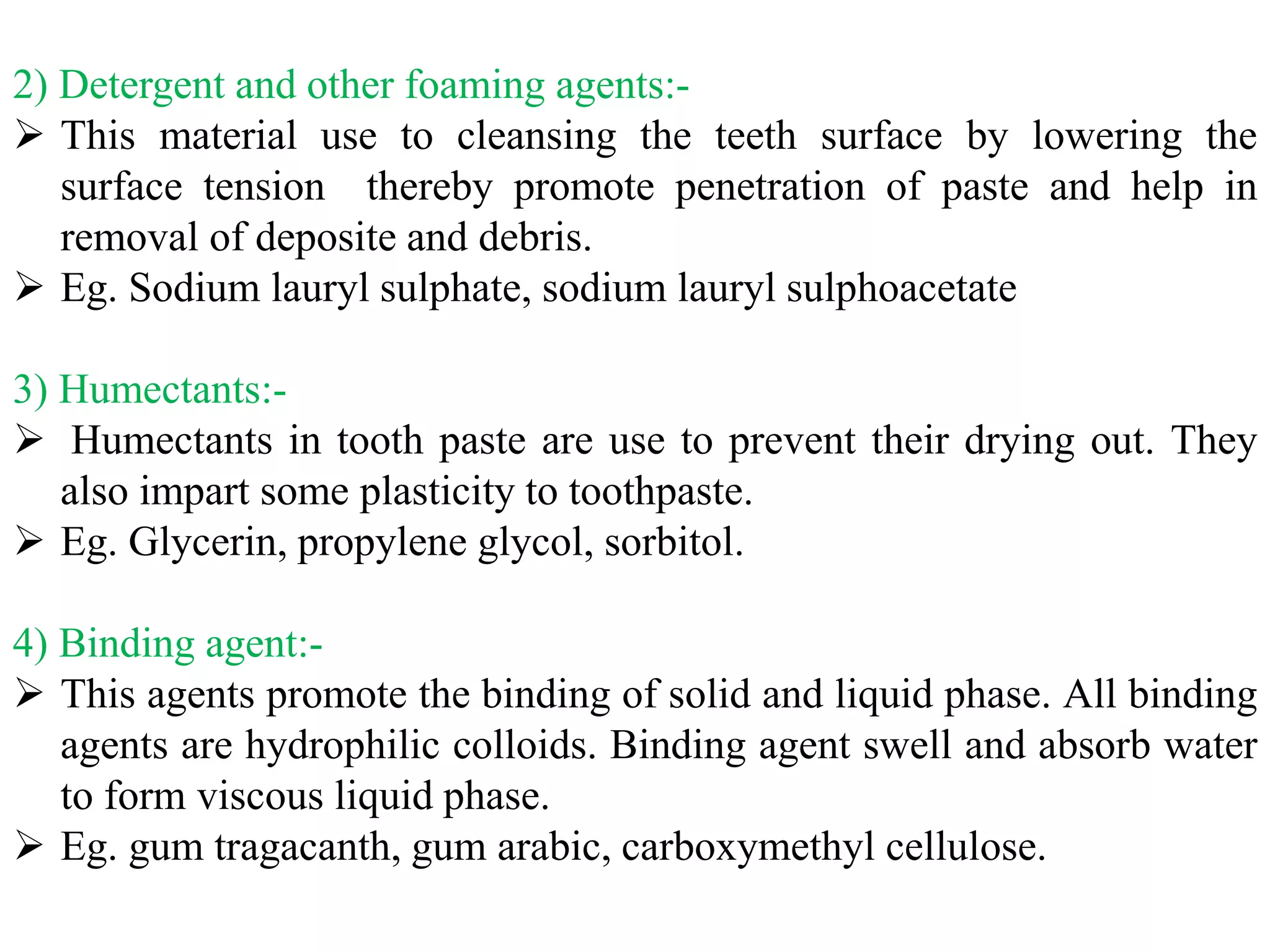
Details various toothpaste ingredients and their functions, ensuring effective cleaning and anti-caries action.
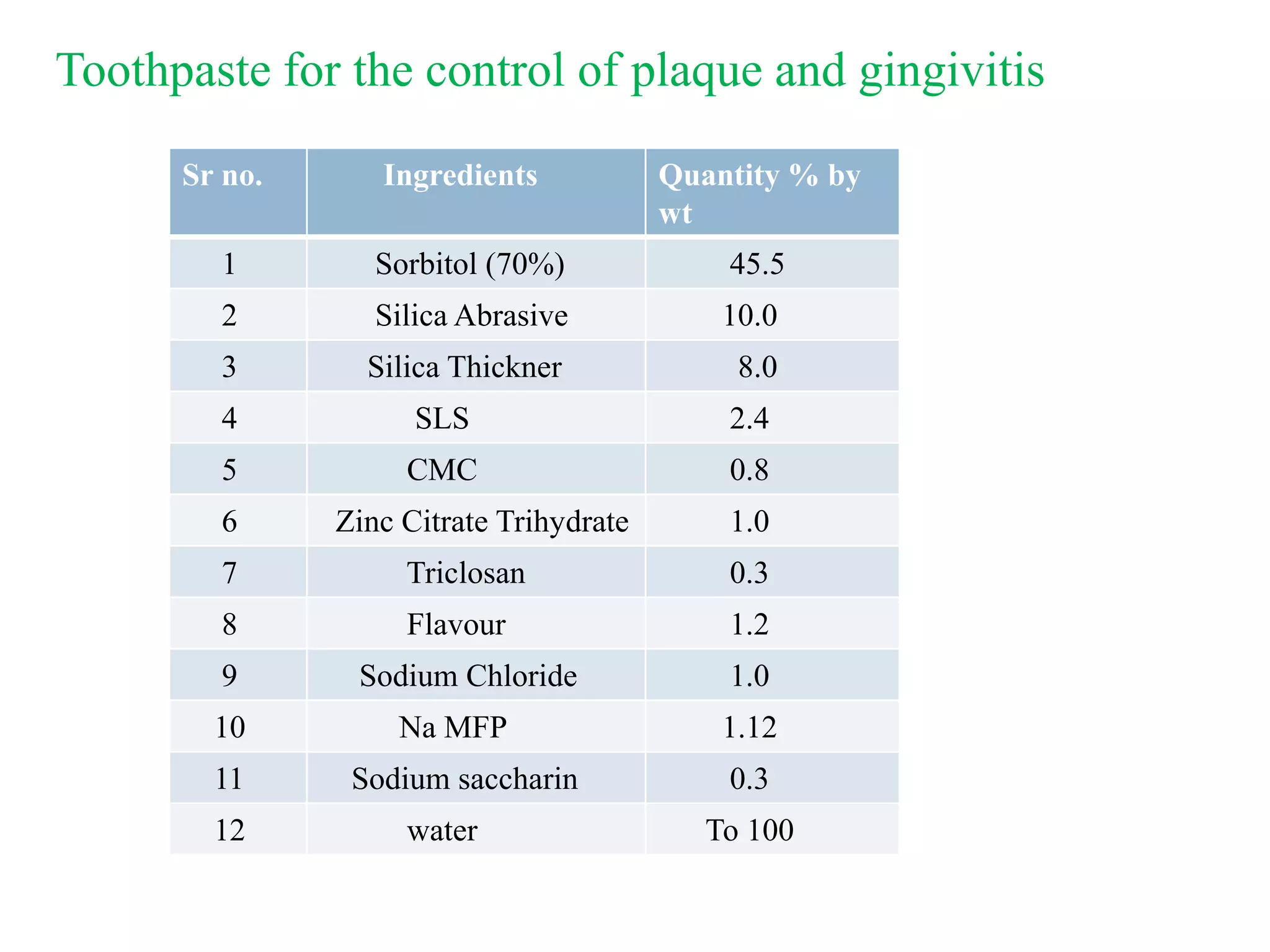
Provides specific ingredient examples and formulations for anticaries and sensitivity toothpastes.
Explains different mouthwash categories and their roles in oral hygiene practices.
Breakdown of key mouthwash components, their functions, and how they contribute to oral health.
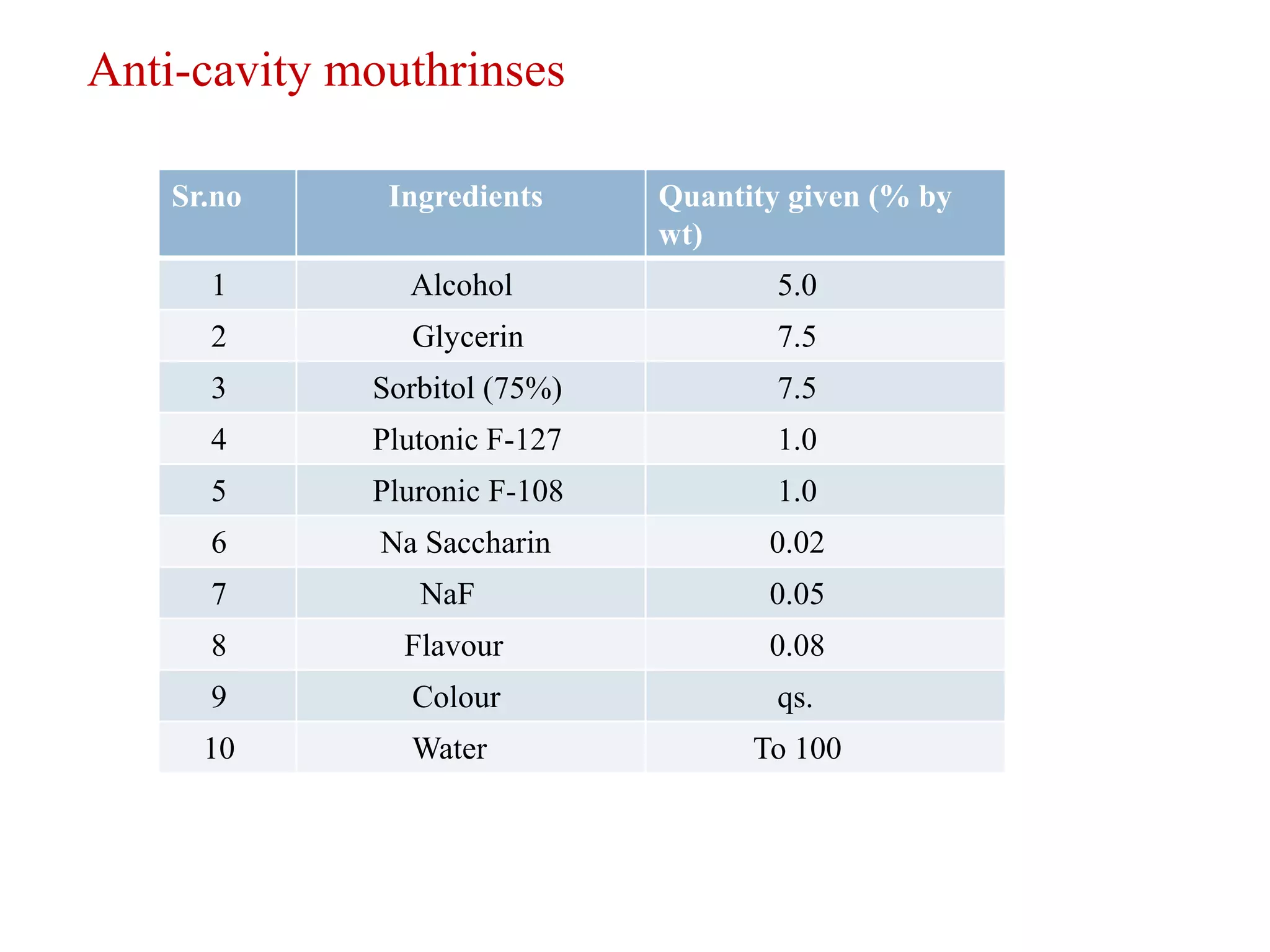
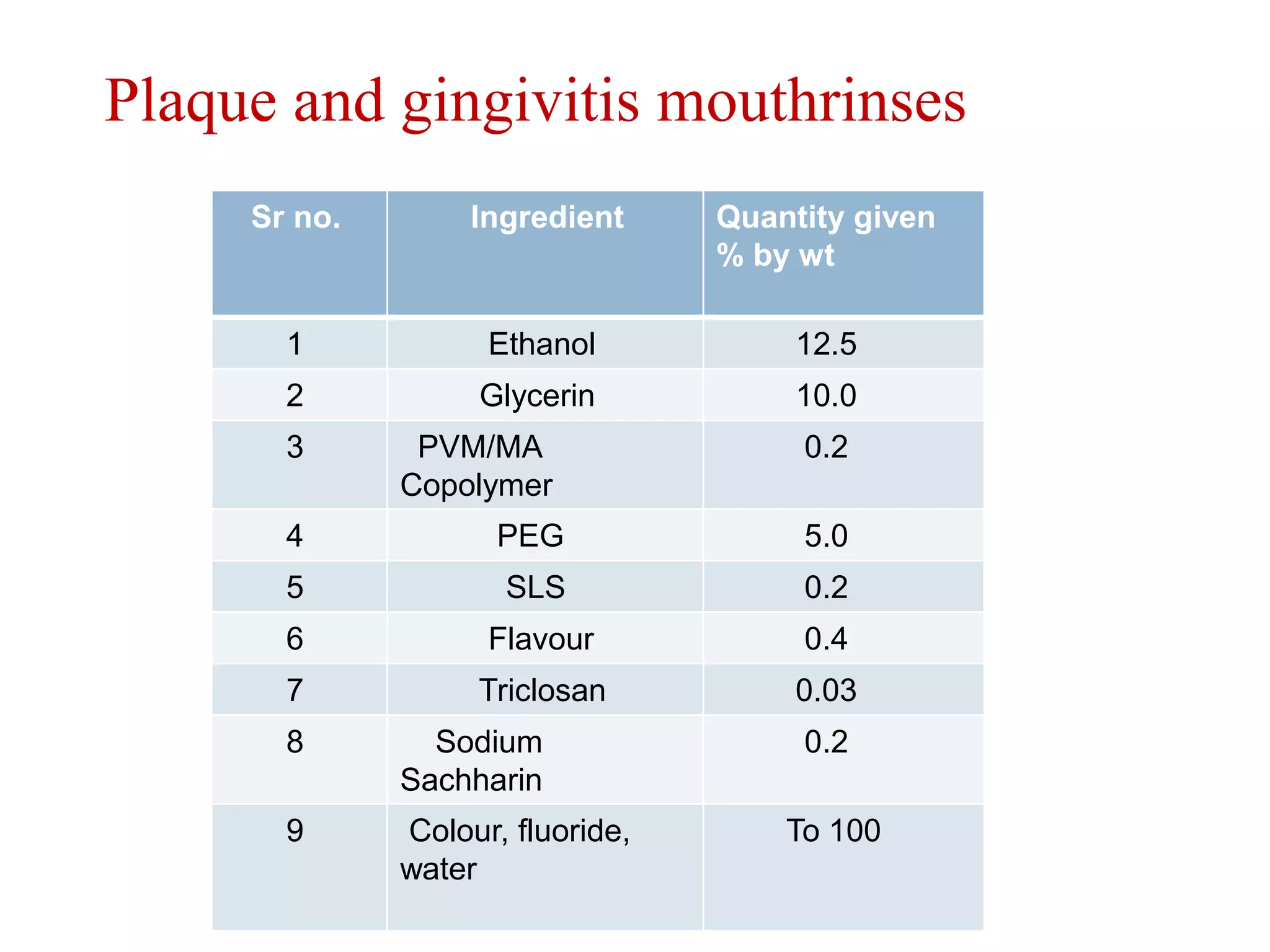
Lists specific formulations and ingredients for anti-cavity and plaque controlling mouthrinses.



















![problems associated with skin[ as per Pharmaceutics]](https://cdn.slidesharecdn.com/ss_thumbnails/2-200204102918-thumbnail.jpg?width=640&height=640&fit=bounds)

































![cosmetics and cosmeticals [department of pharmaceutics]](https://cdn.slidesharecdn.com/ss_thumbnails/1-200204101110-thumbnail.jpg?width=640&height=640&fit=bounds)
![MUTUAL PRODRUG [PHARMACEUTICALS]](https://cdn.slidesharecdn.com/ss_thumbnails/67-191220064837-thumbnail.jpg?width=640&height=640&fit=bounds)
![TITANIUM CHLORIDE [PHARMACEUTICAL REAGENT]](https://cdn.slidesharecdn.com/ss_thumbnails/66-191220064235-thumbnail.jpg?width=640&height=640&fit=bounds)
![OLIGONUCLEOTIDE THERAPY [ TECHNIQUES, APPLICATIONS]](https://cdn.slidesharecdn.com/ss_thumbnails/66-191220063512-thumbnail.jpg?width=640&height=640&fit=bounds)
![OXIDATION [PHARMACEUTICAL PROCESS CHEMISTRY]](https://cdn.slidesharecdn.com/ss_thumbnails/65-191220062805-thumbnail.jpg?width=640&height=640&fit=bounds)

![PHASE TRANSFER CATALYSIS [PTC]](https://cdn.slidesharecdn.com/ss_thumbnails/64-191219161253-thumbnail.jpg?width=640&height=640&fit=bounds)

![LIQUID CHROMATOGRAPHY- MASS SPECTROSCOPY[LC-MS]](https://cdn.slidesharecdn.com/ss_thumbnails/63-191219160156-thumbnail.jpg?width=640&height=640&fit=bounds)

![Homogeneous catalysis [ MPHARM, MSC, BPHARM, BSC]](https://cdn.slidesharecdn.com/ss_thumbnails/62-191219155346-thumbnail.jpg?width=640&height=640&fit=bounds)
![Dicyclohexylcarbodiimide [DCC]](https://cdn.slidesharecdn.com/ss_thumbnails/61-191219150428-thumbnail.jpg?width=640&height=640&fit=bounds)

![GREEN CHEMISTRY [IS A SOLUTION TO ENVIRONMENT PROBLEM?]](https://cdn.slidesharecdn.com/ss_thumbnails/60-191219142616-thumbnail.jpg?width=640&height=640&fit=bounds)




















