Downloaded 358 times
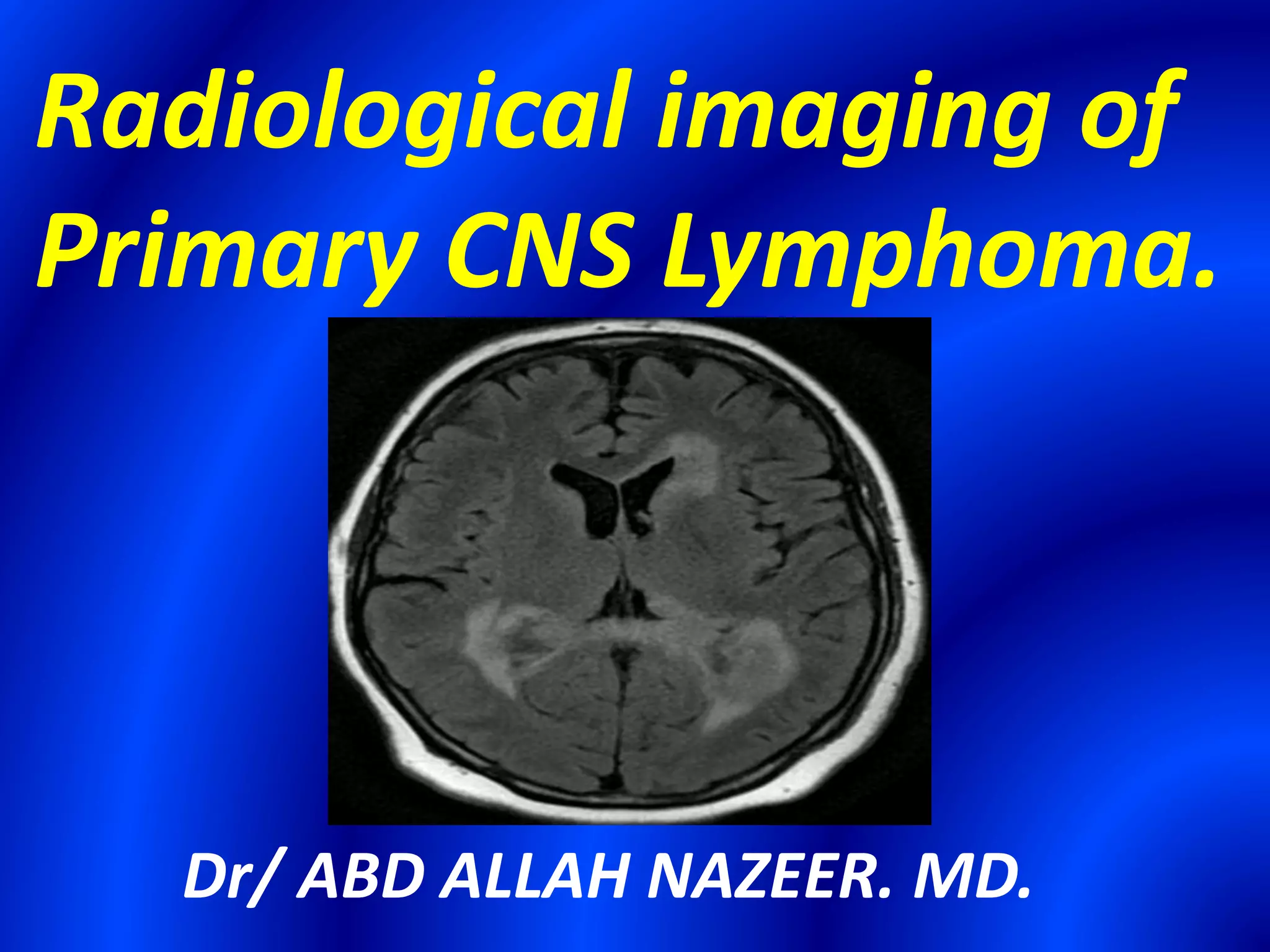
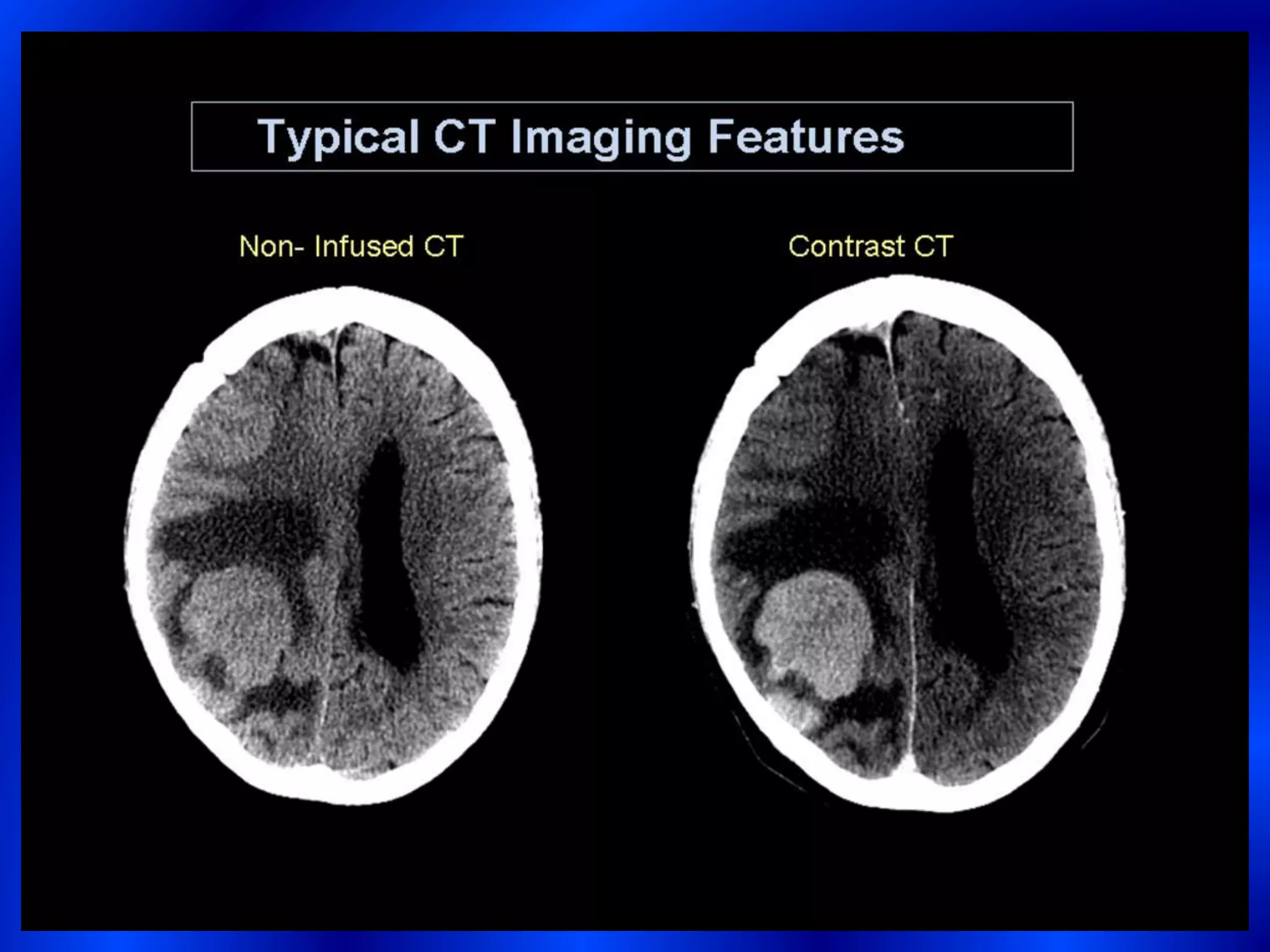
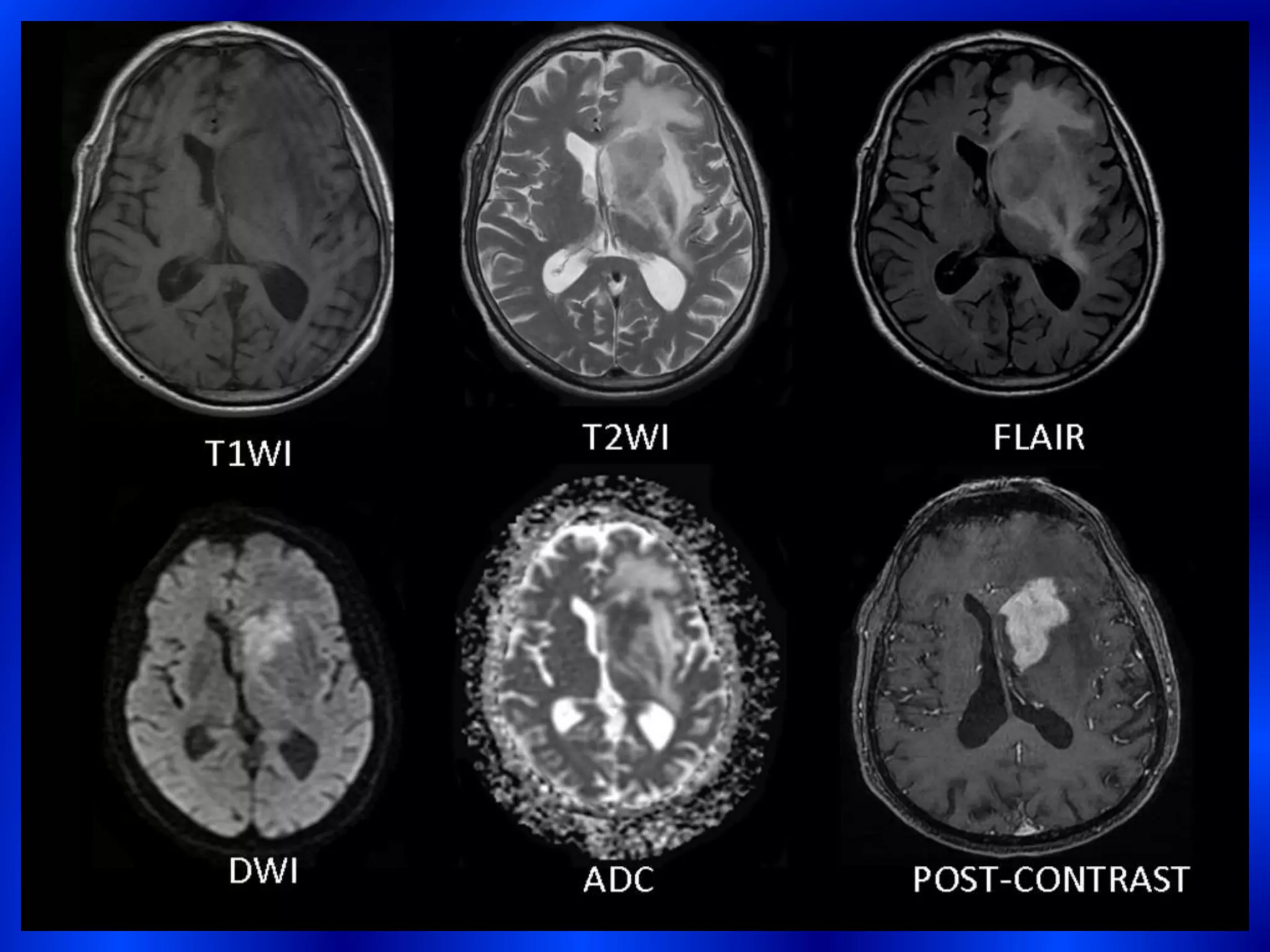

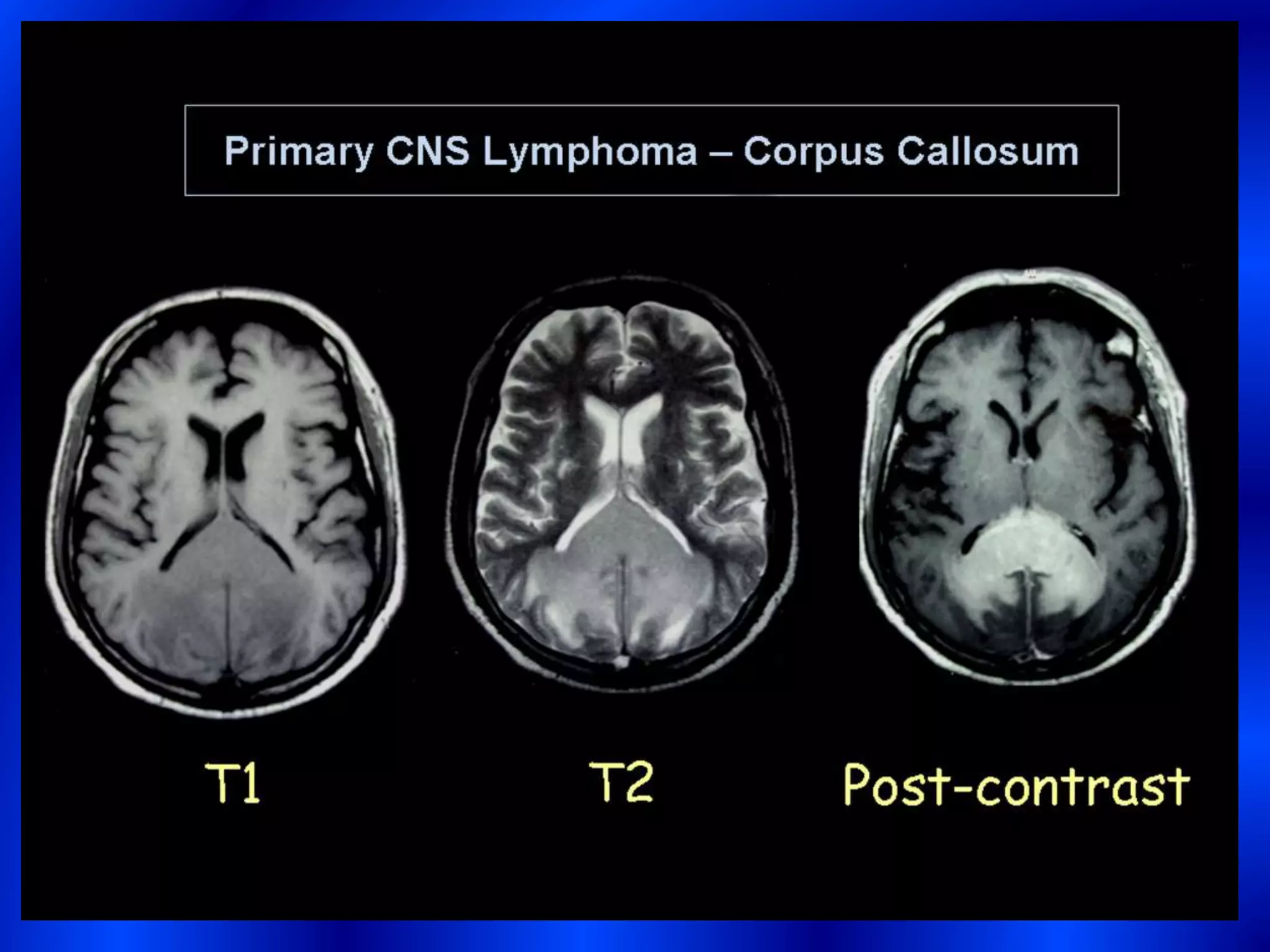
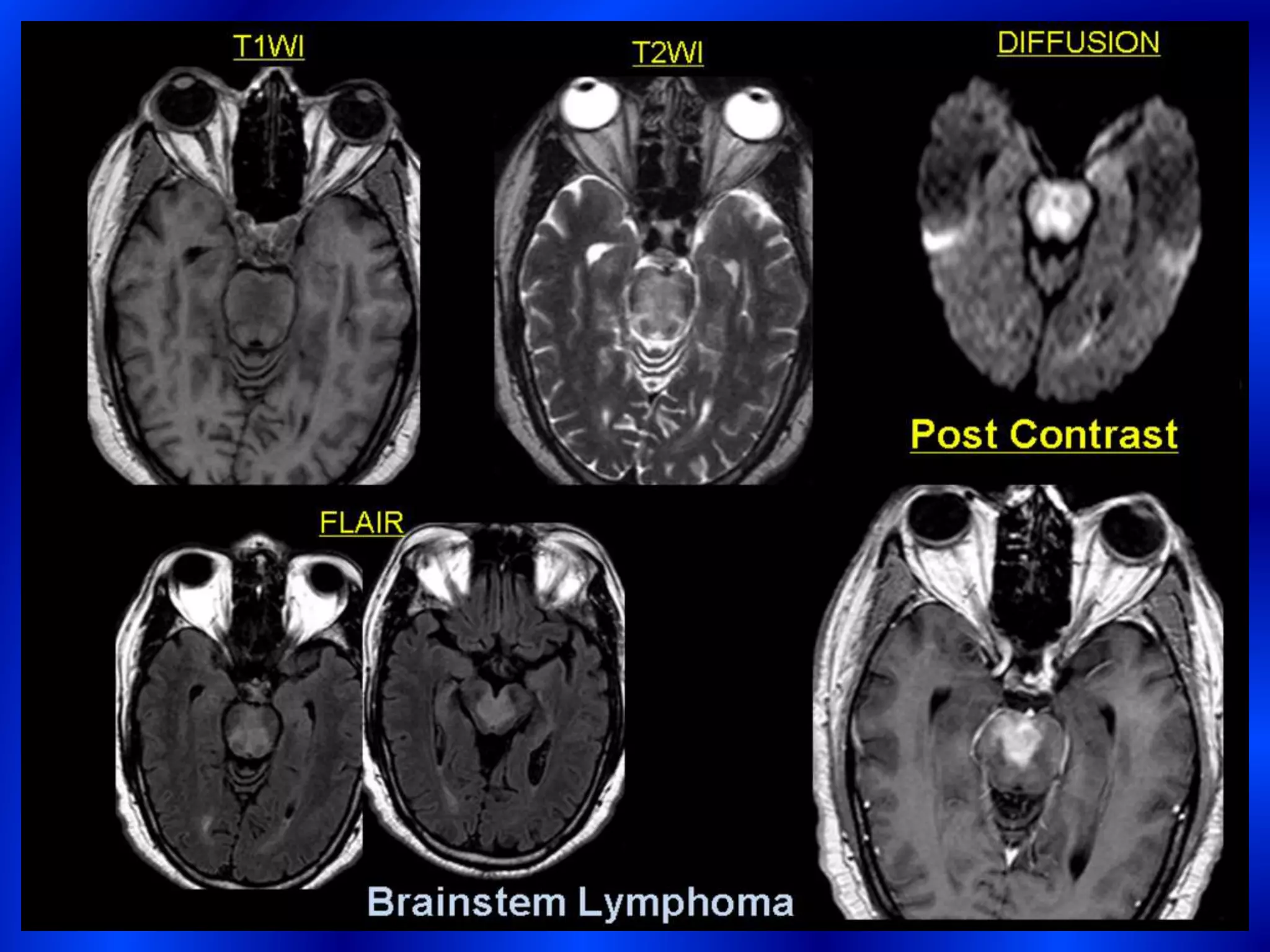
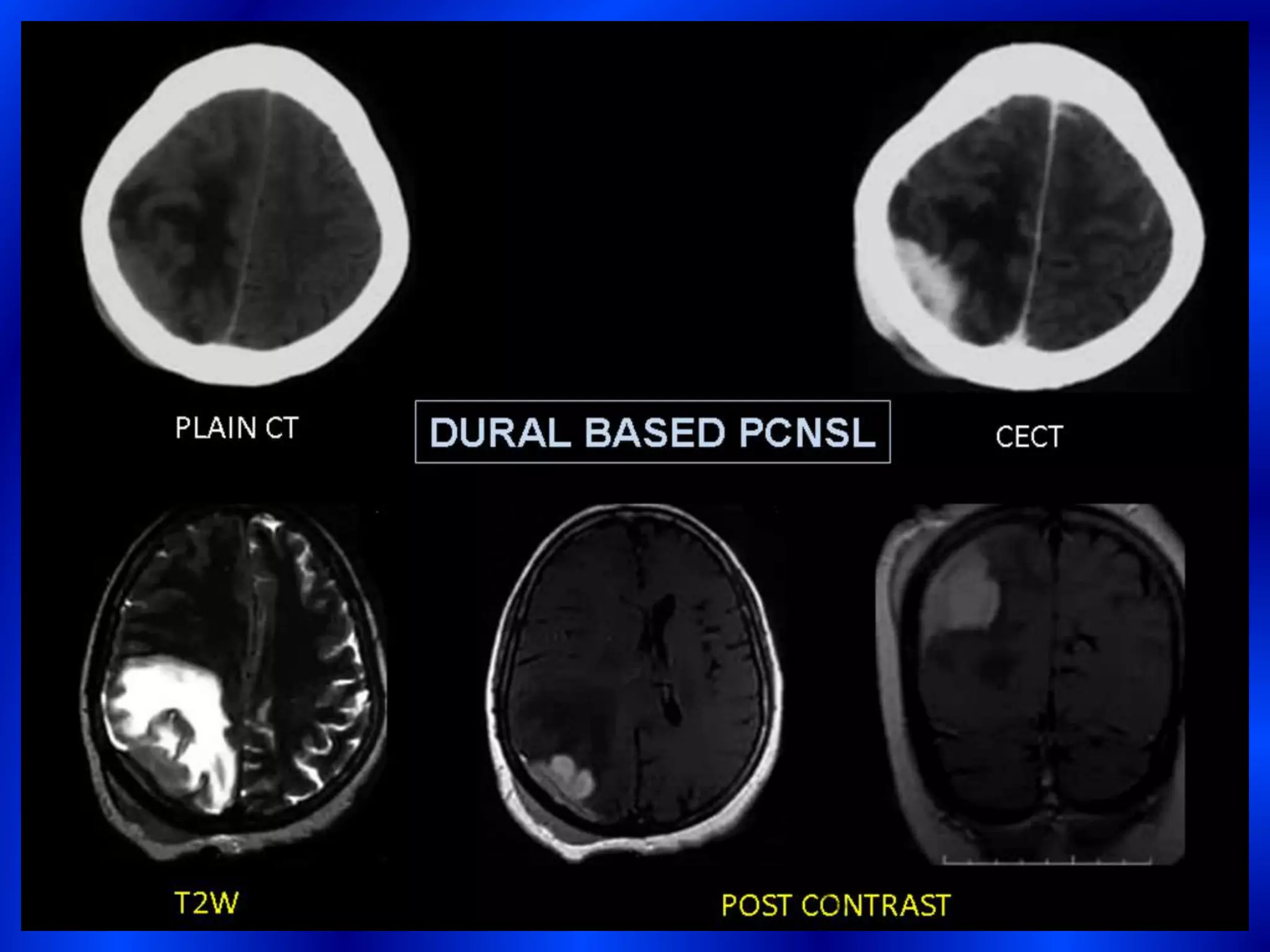
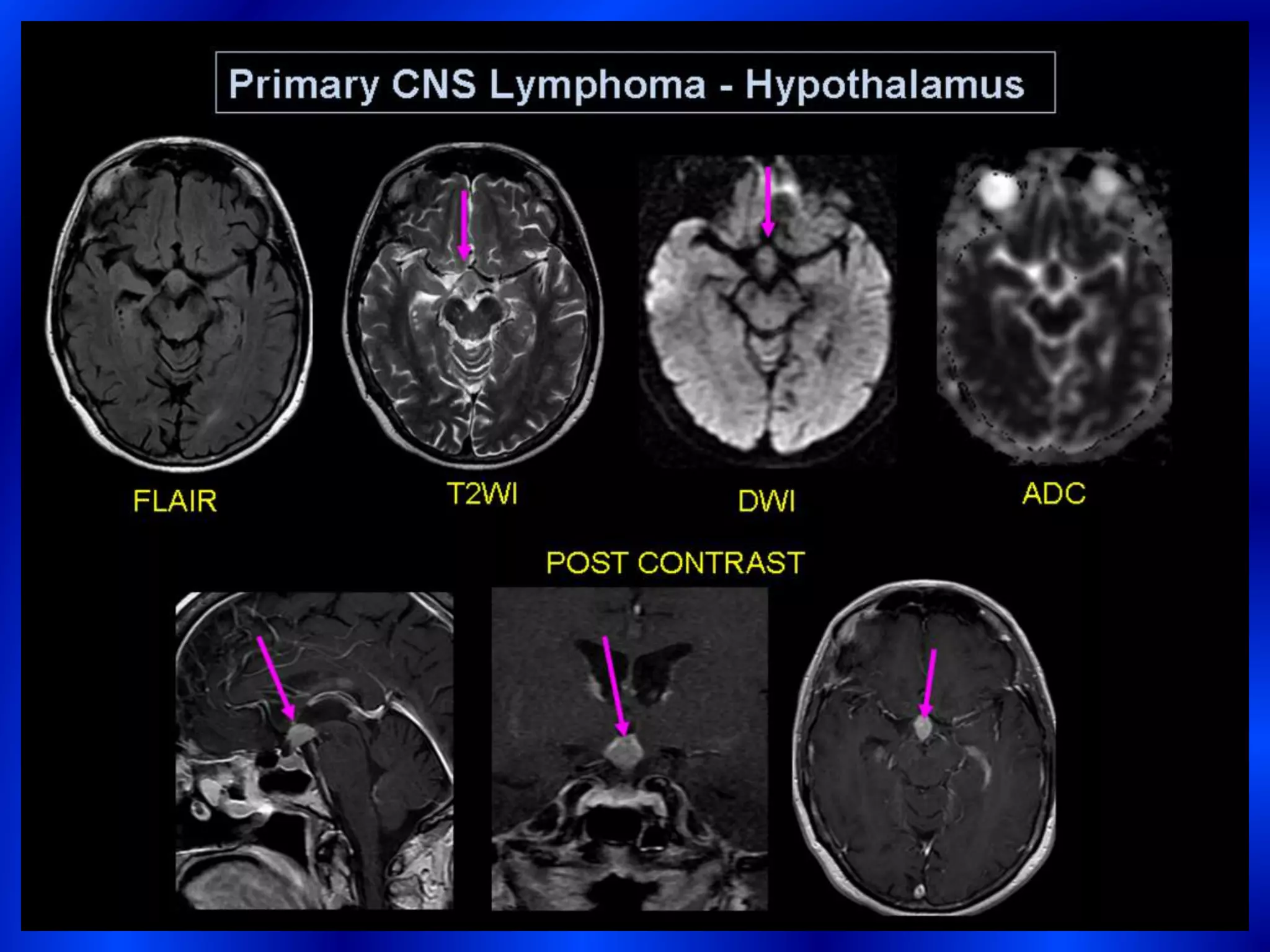
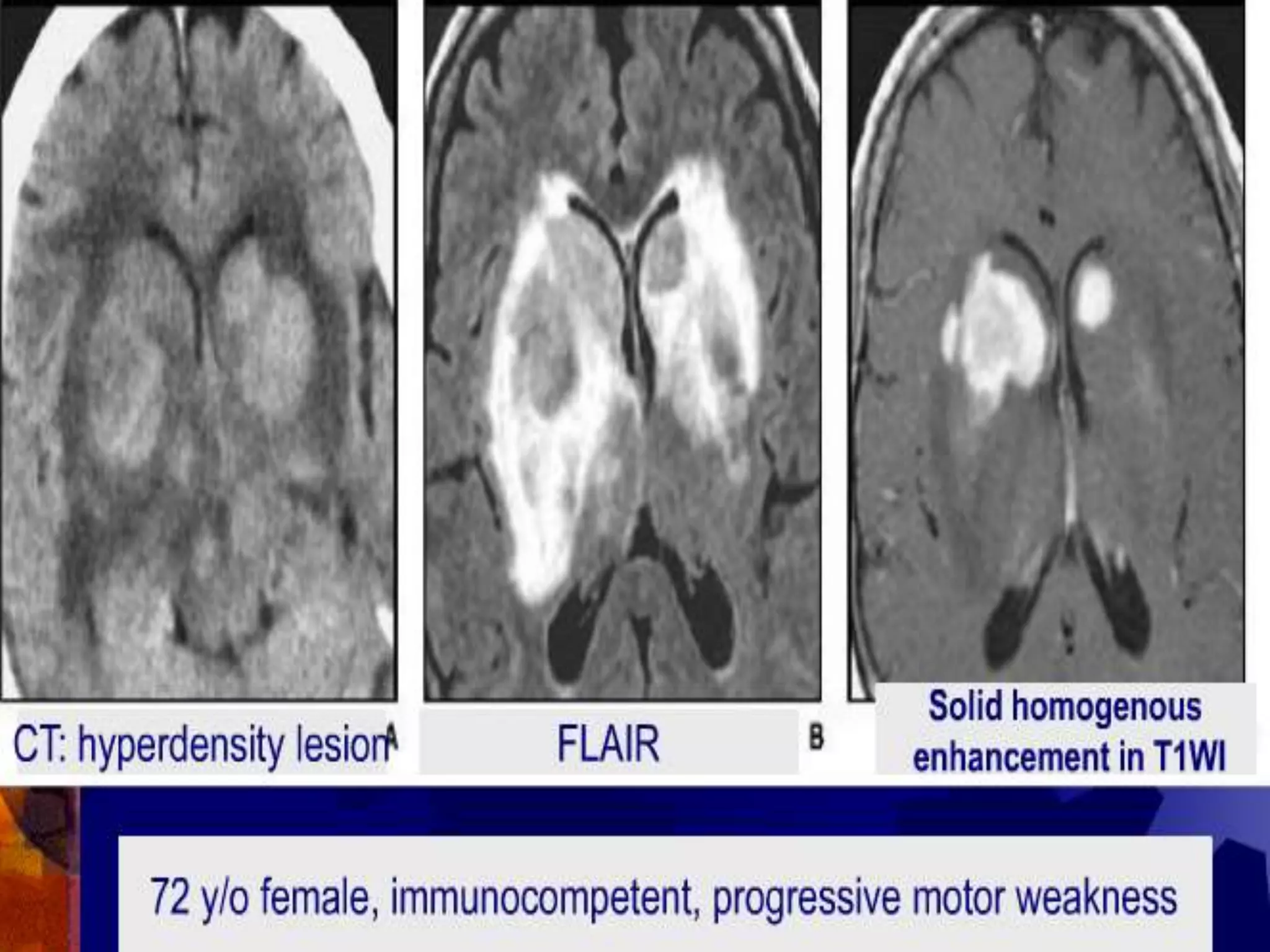
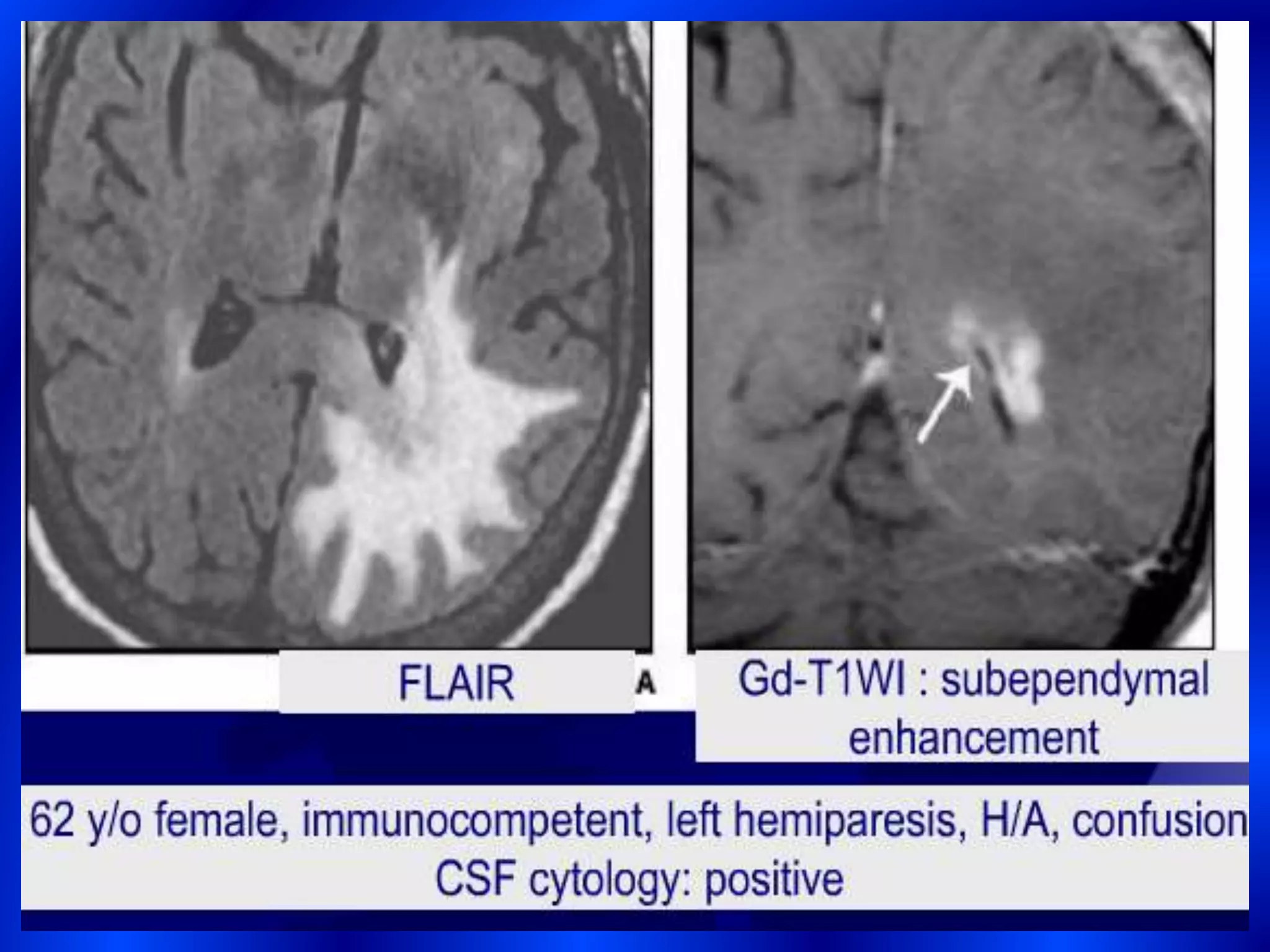
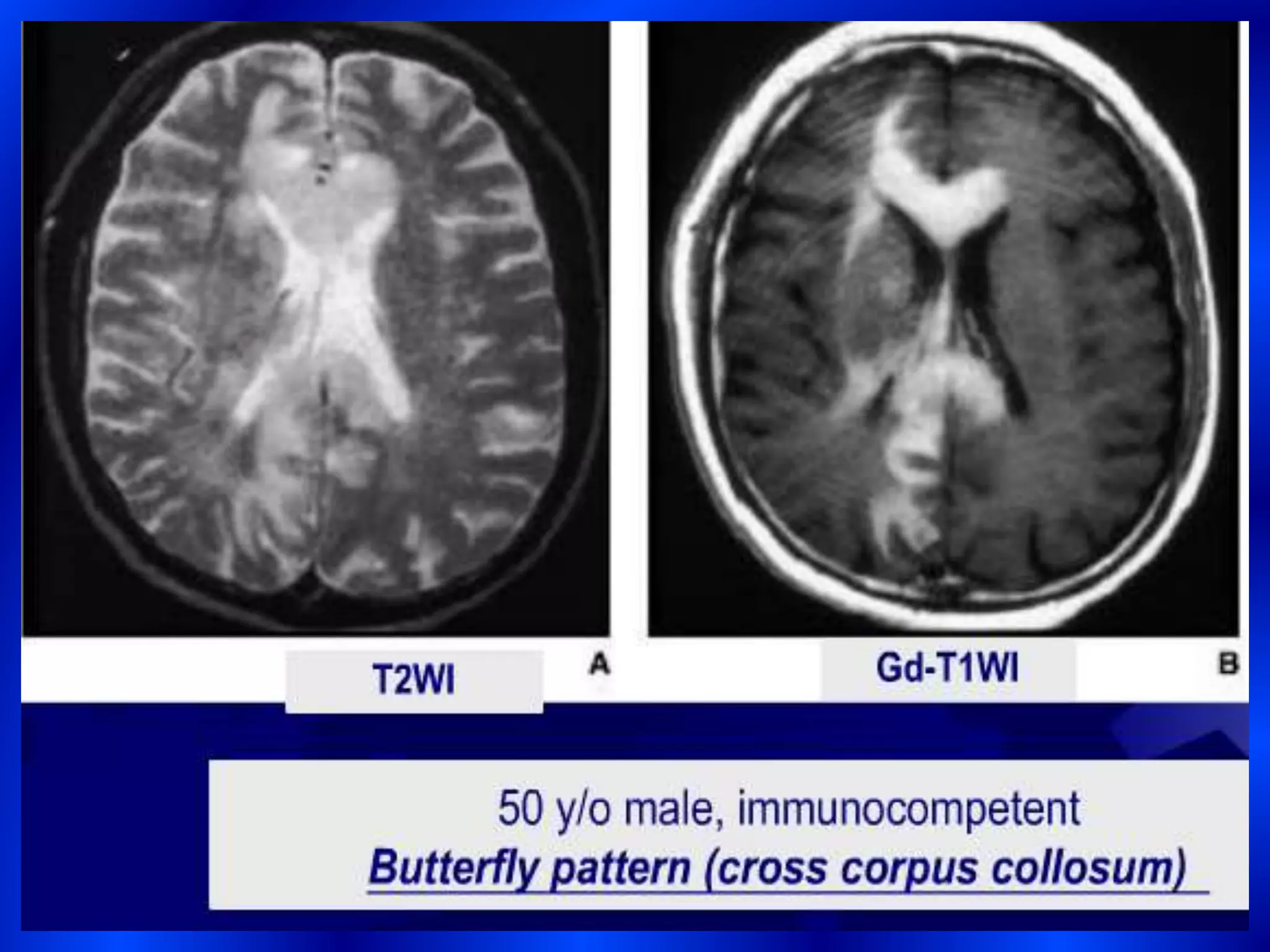
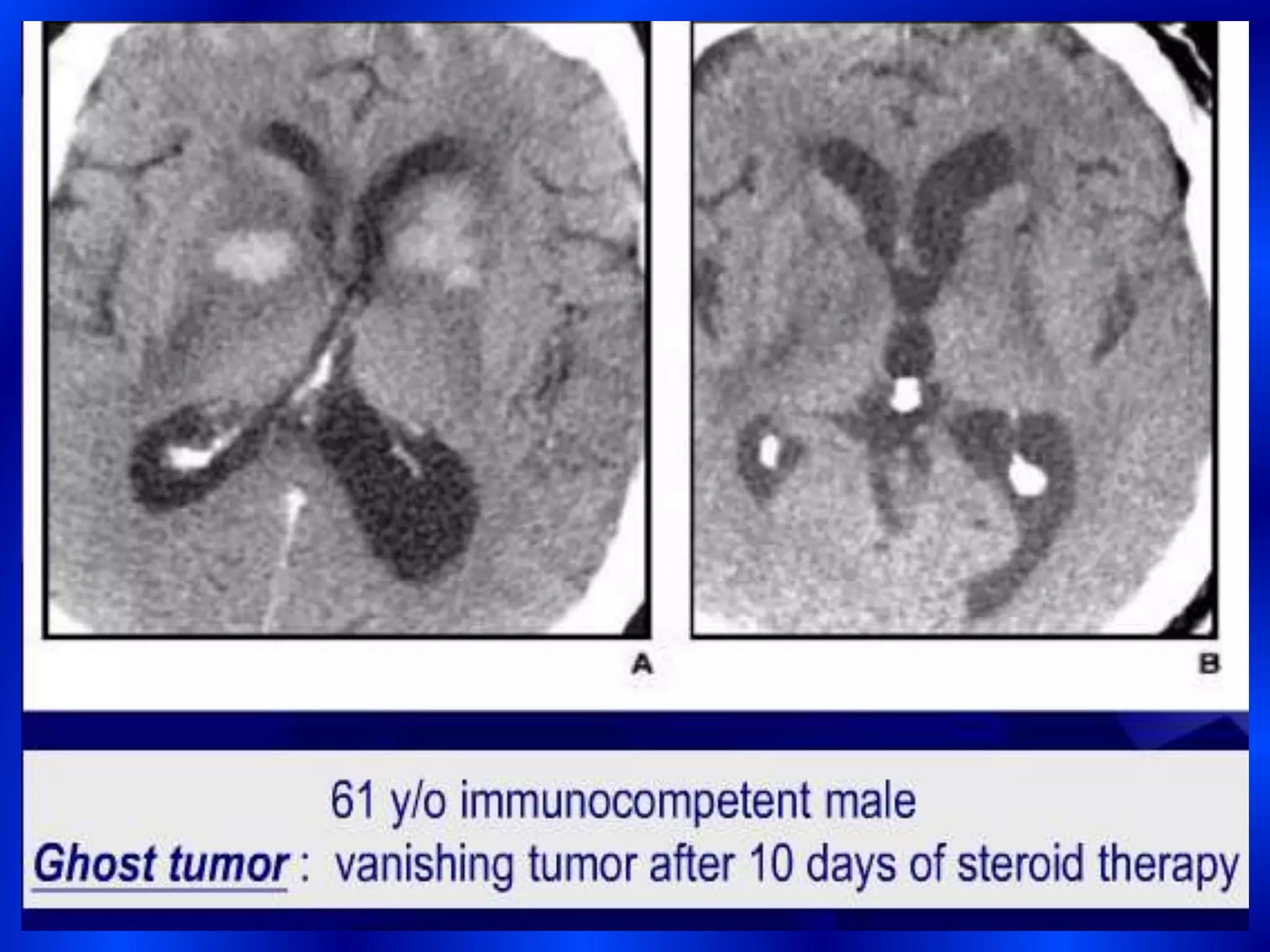
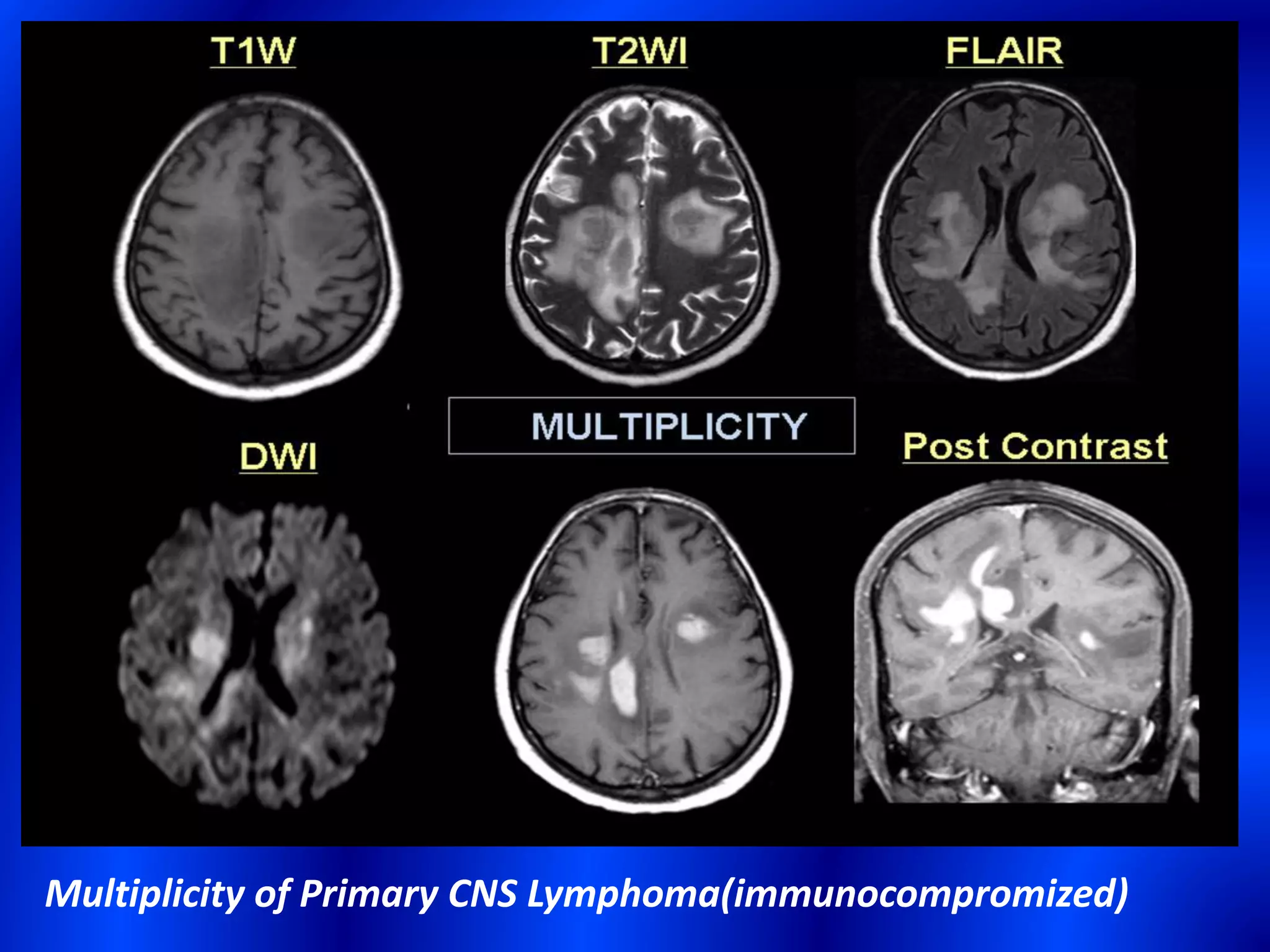
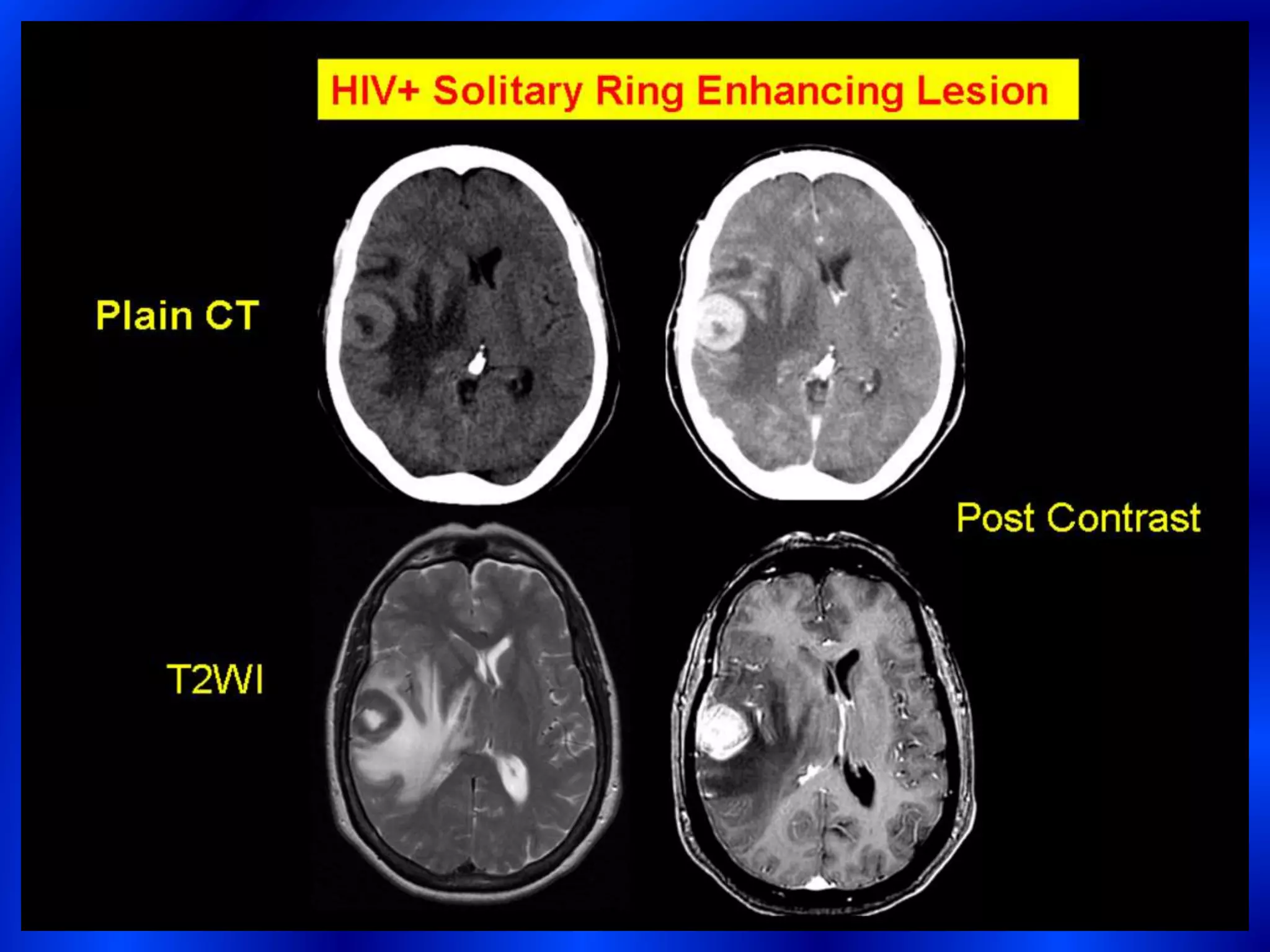
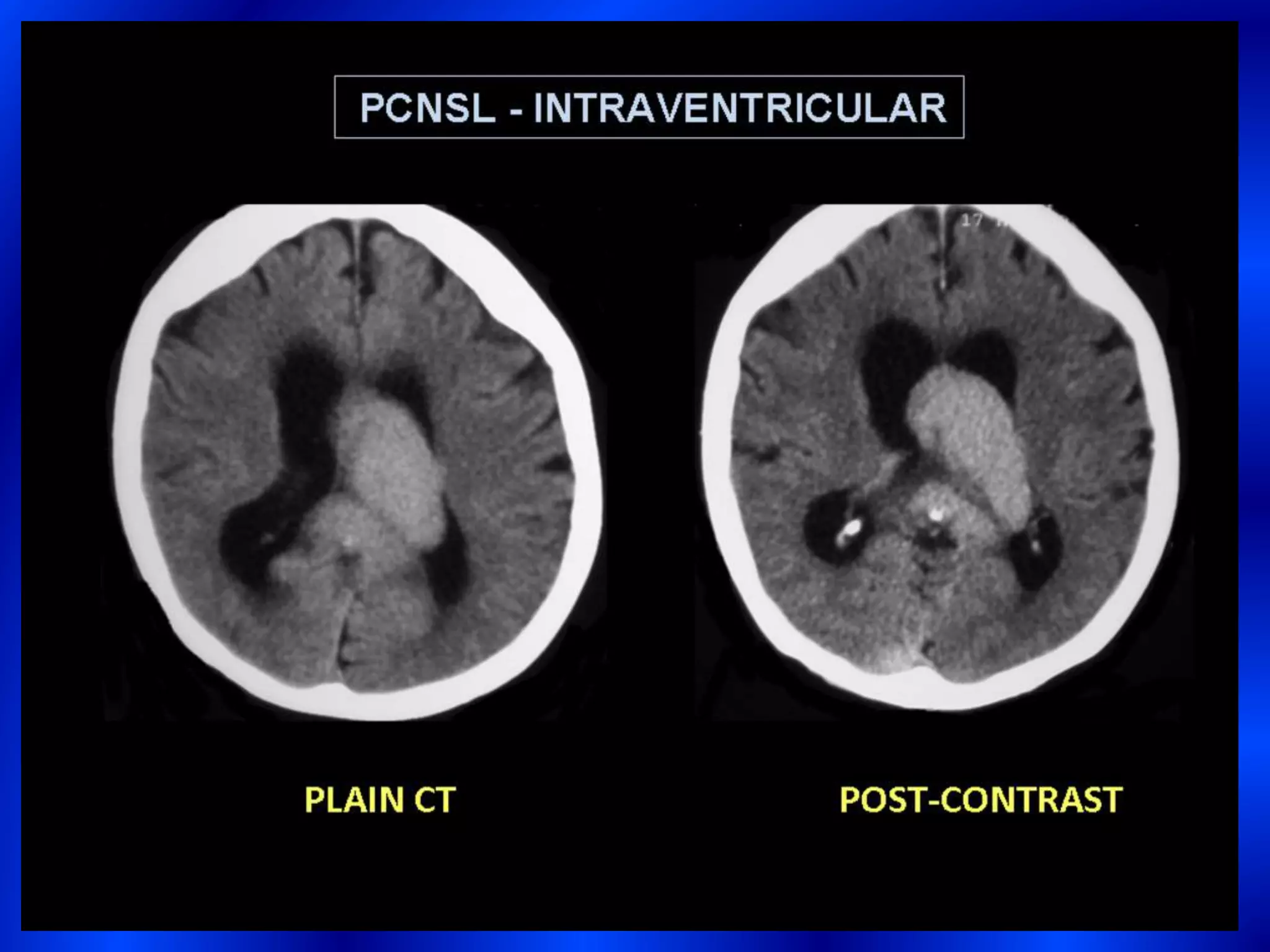
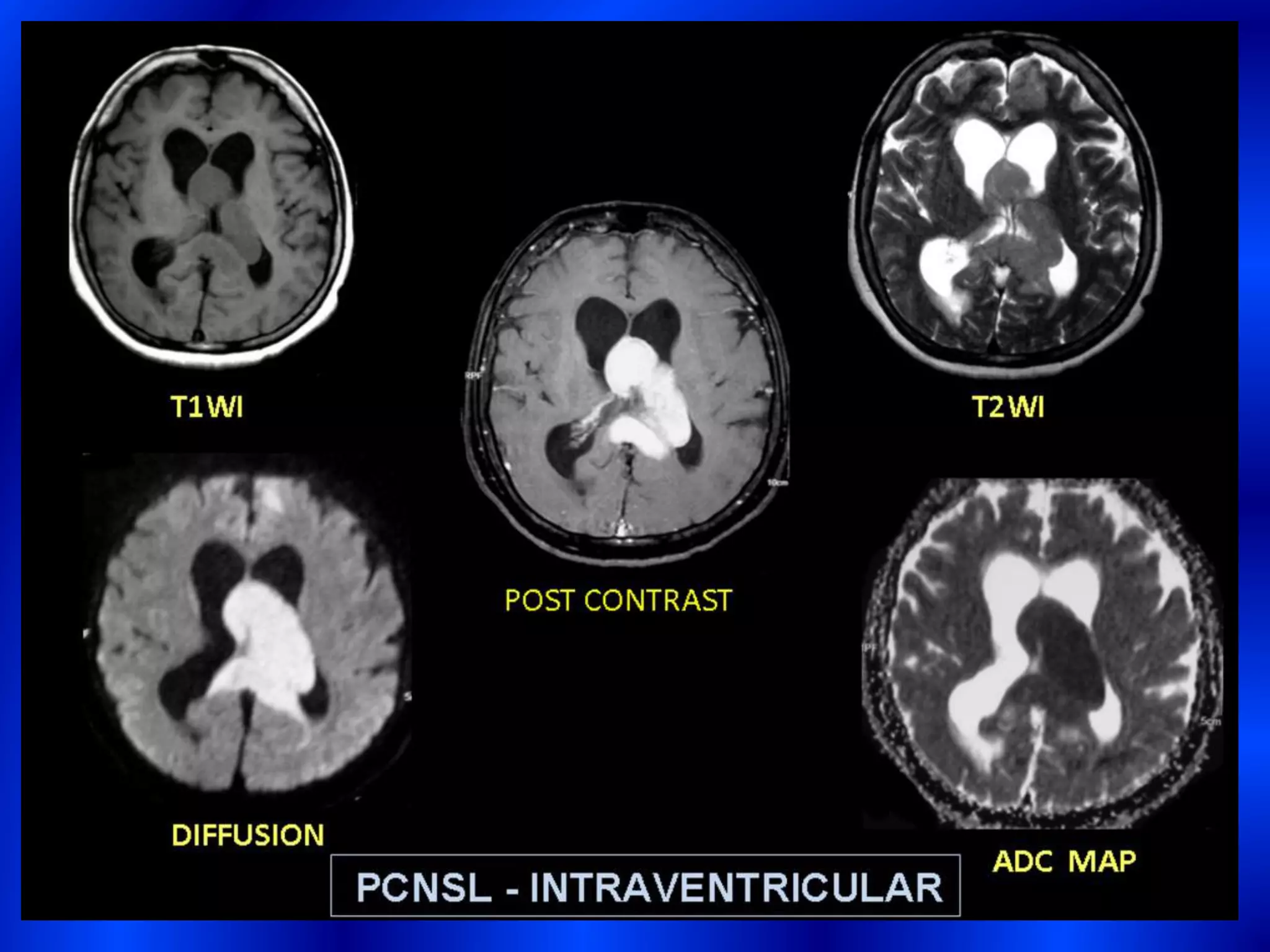
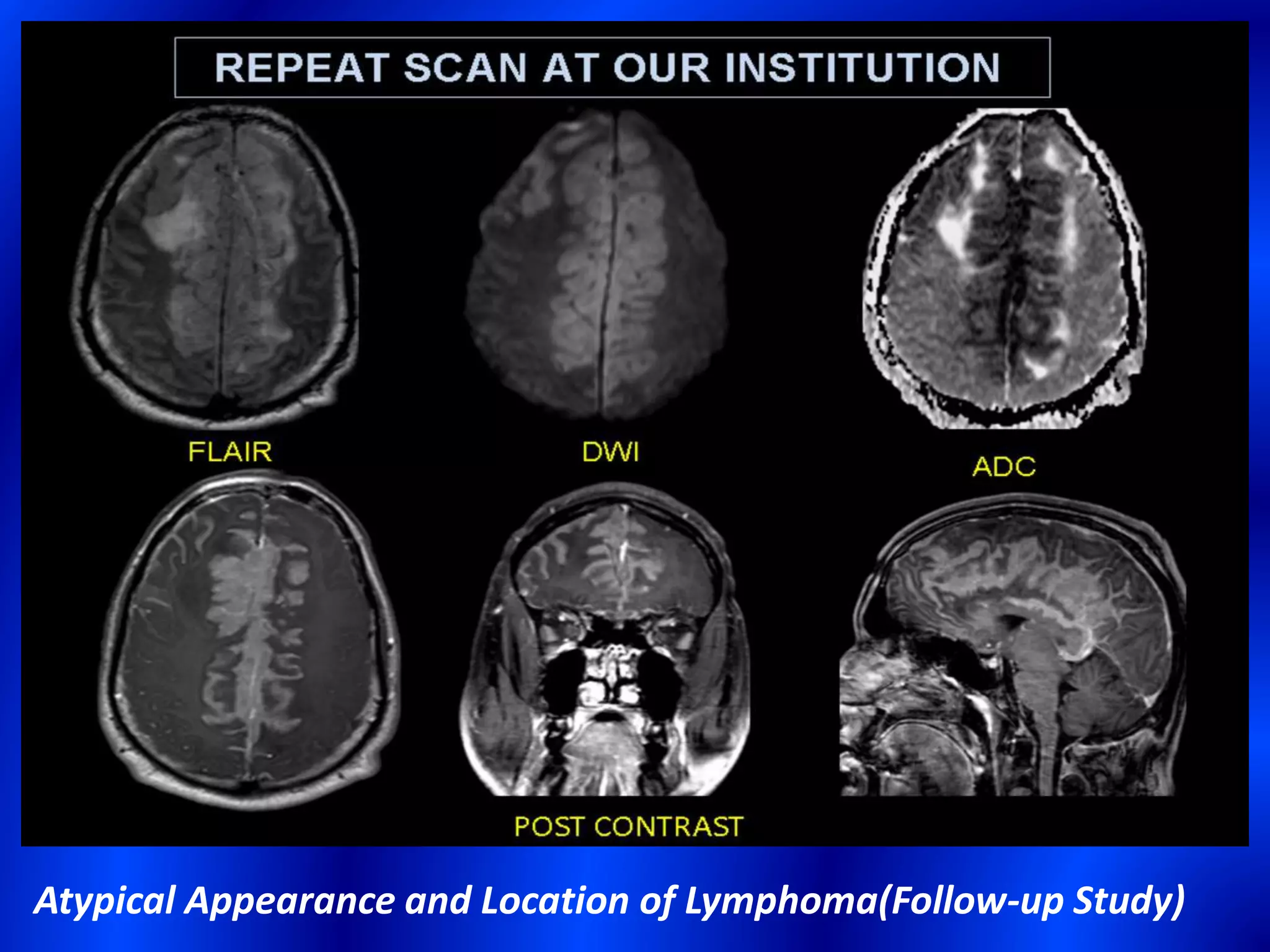
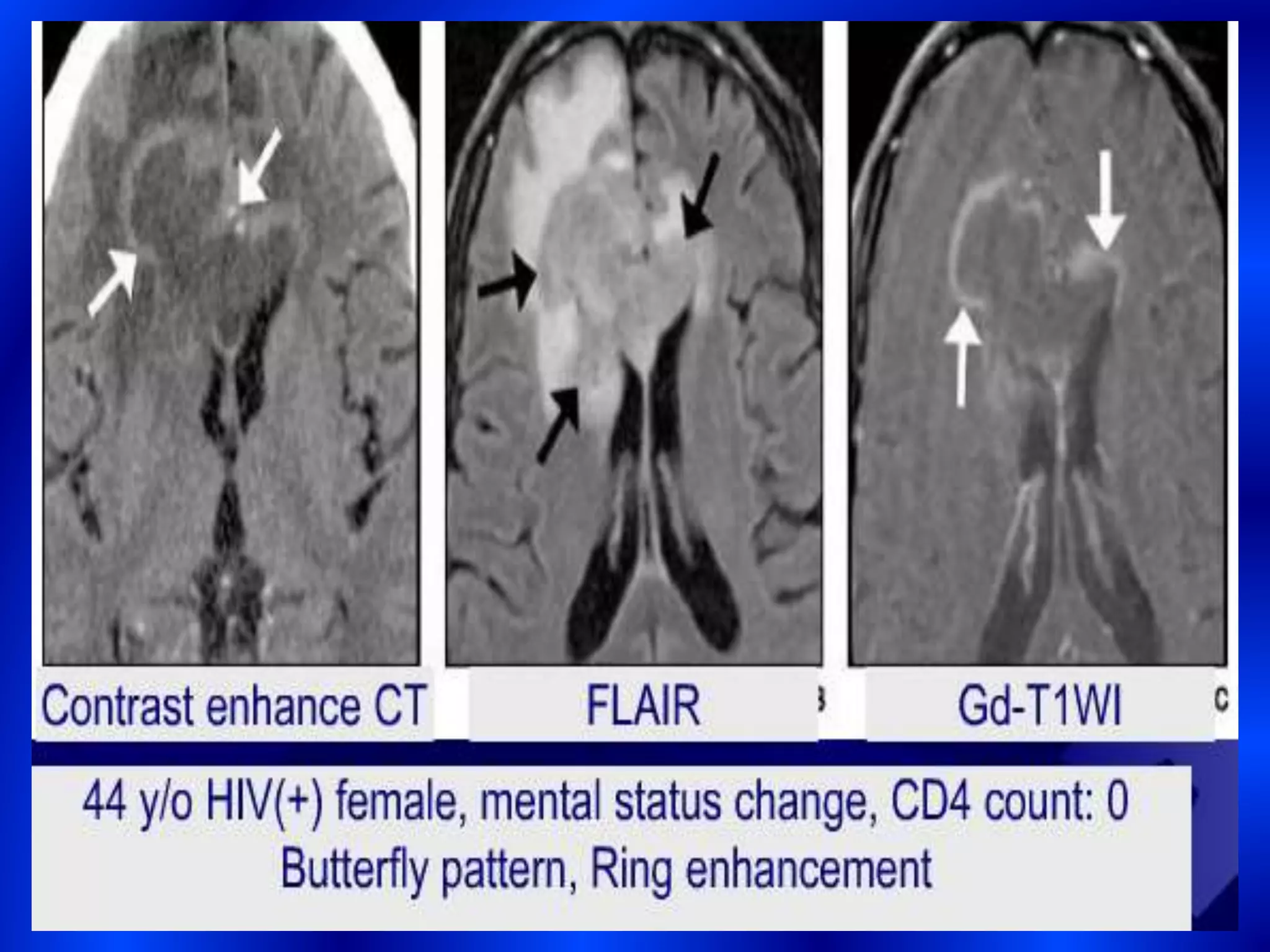
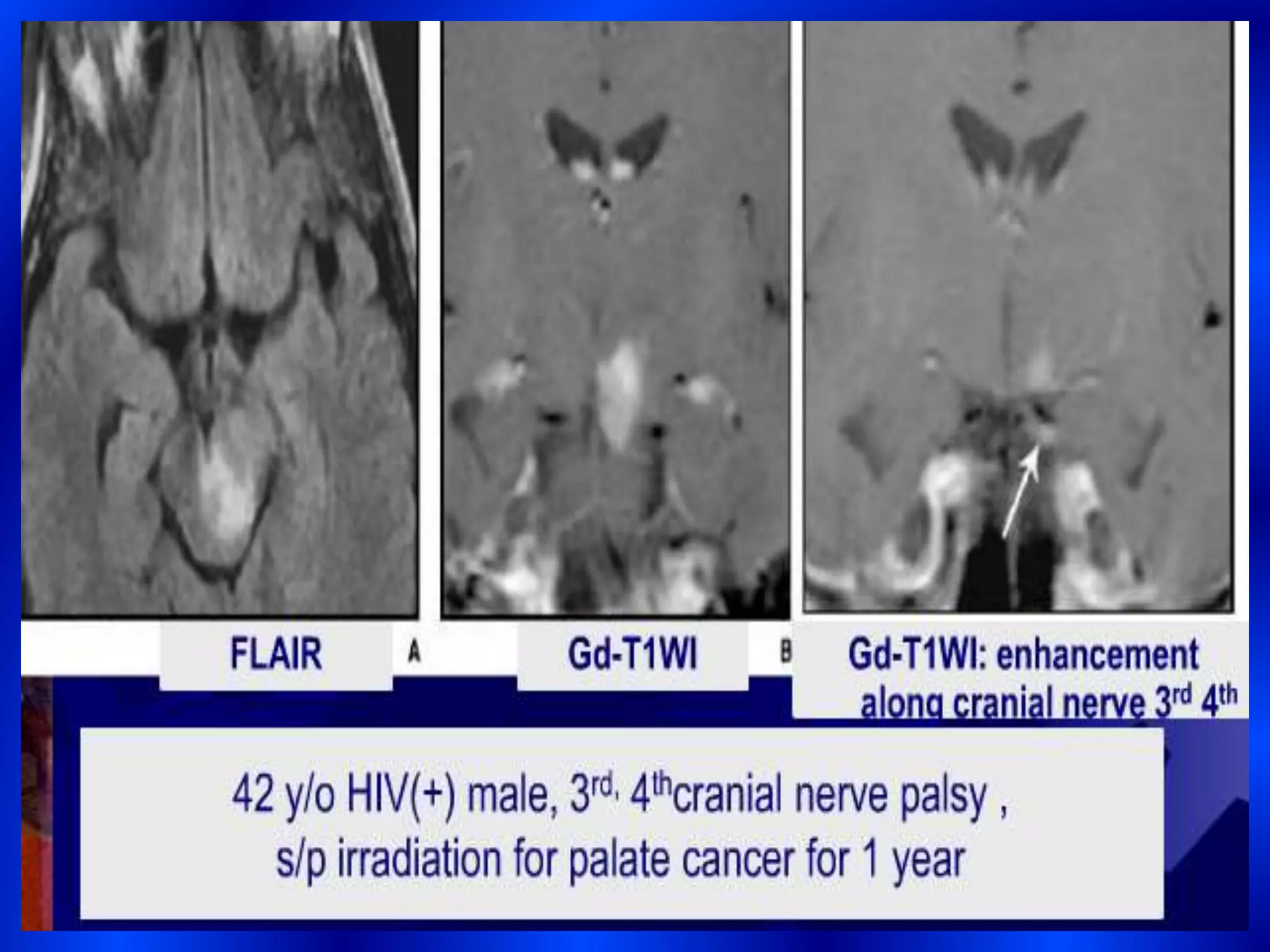
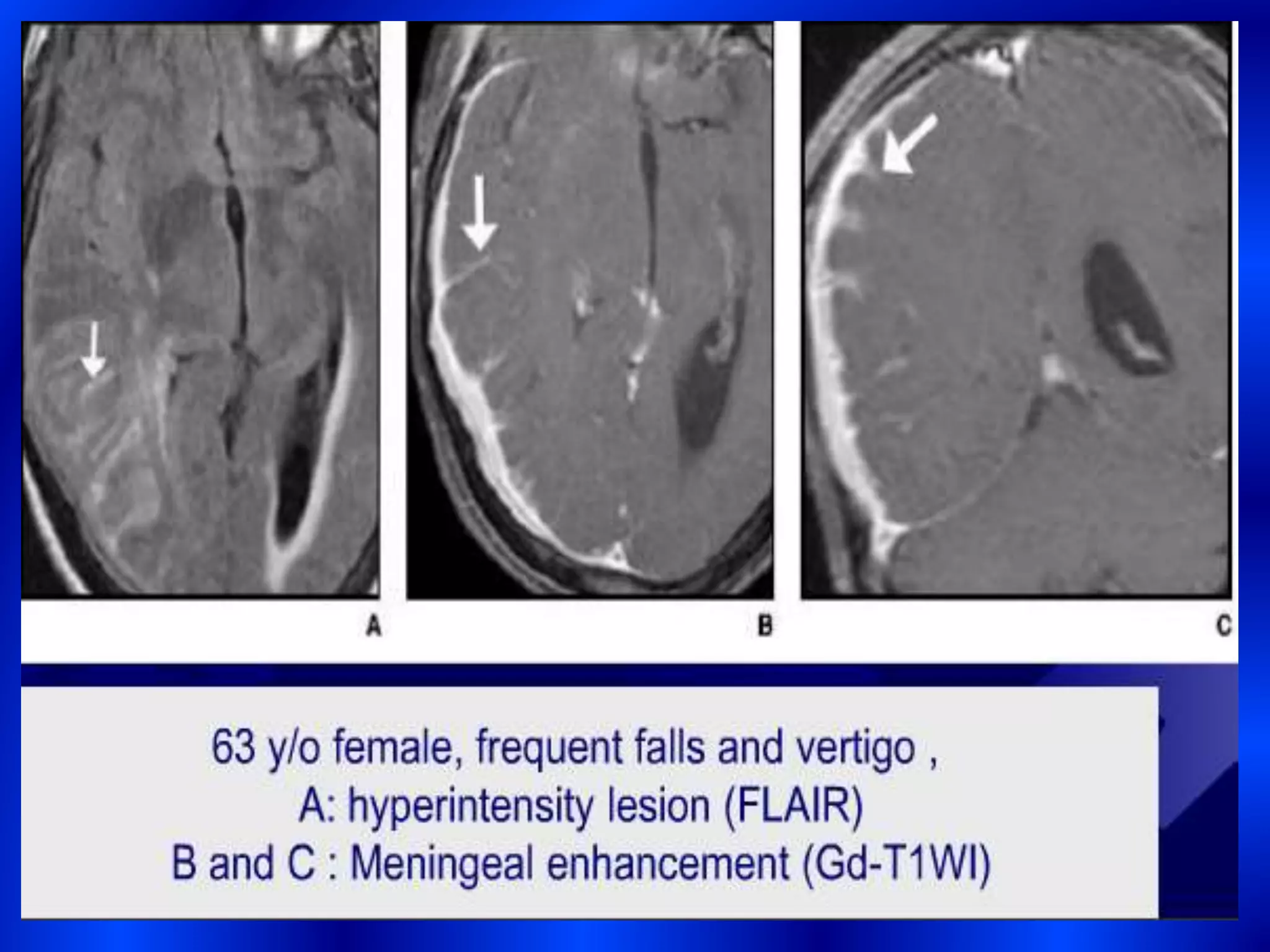
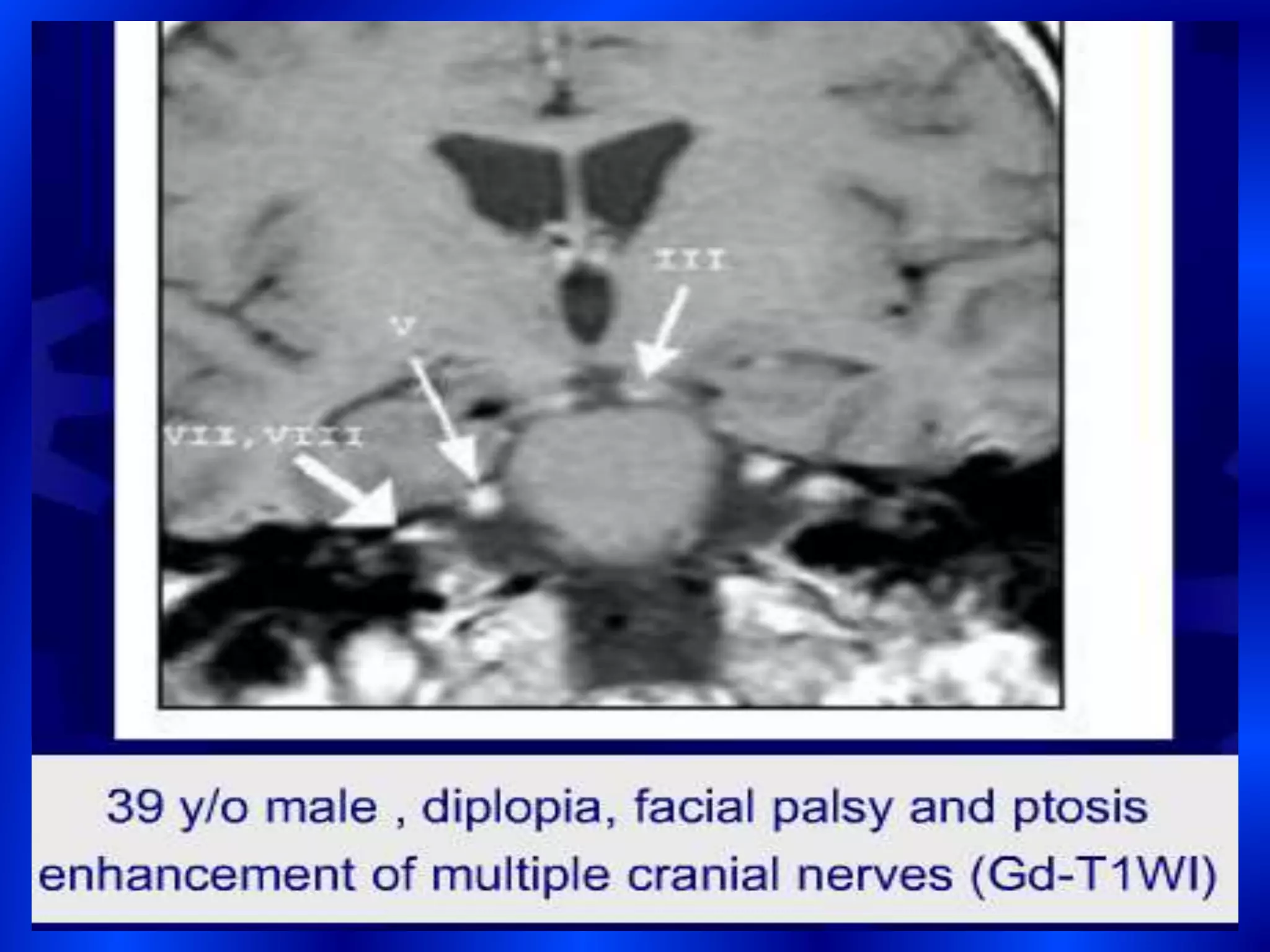
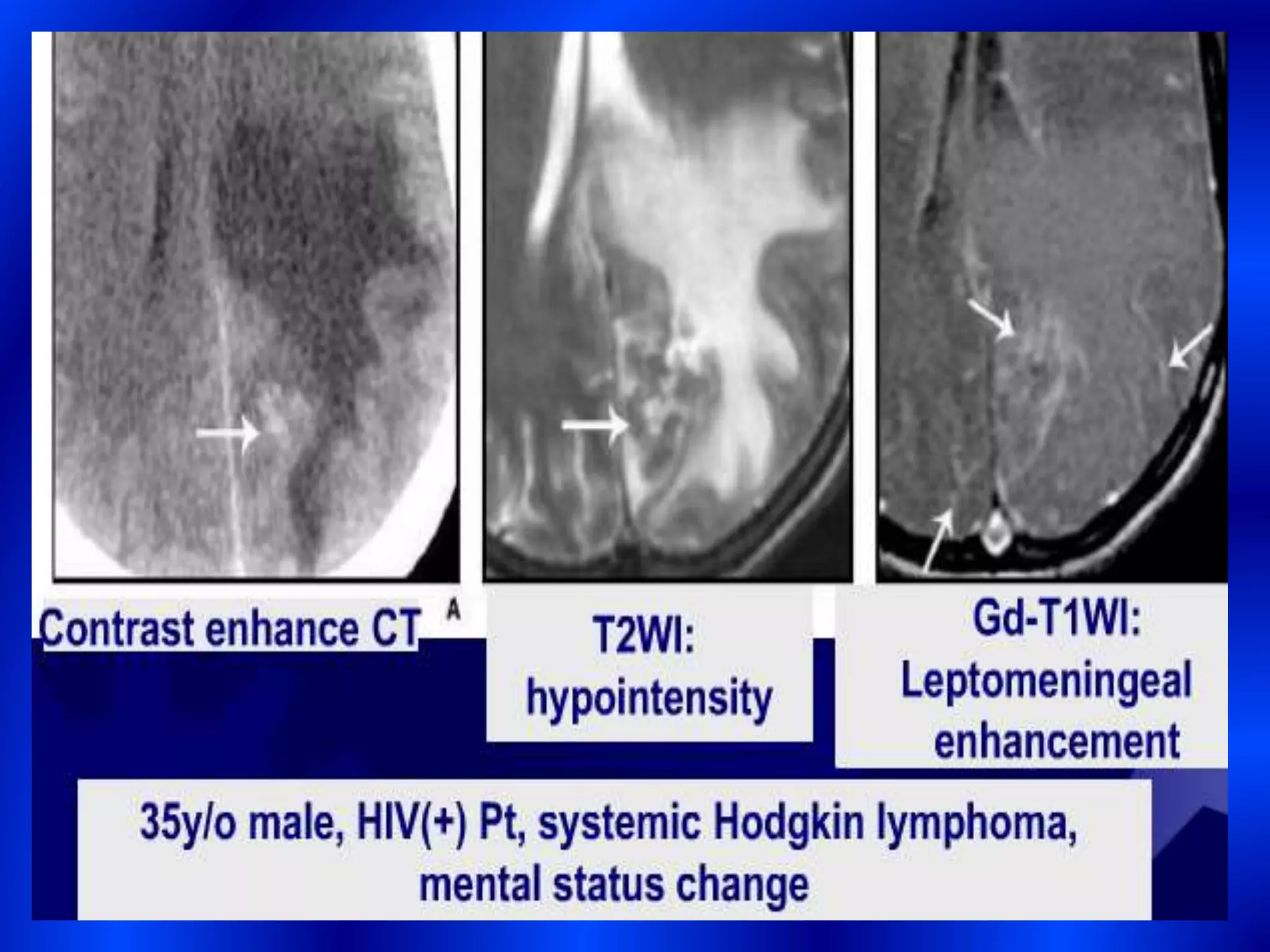
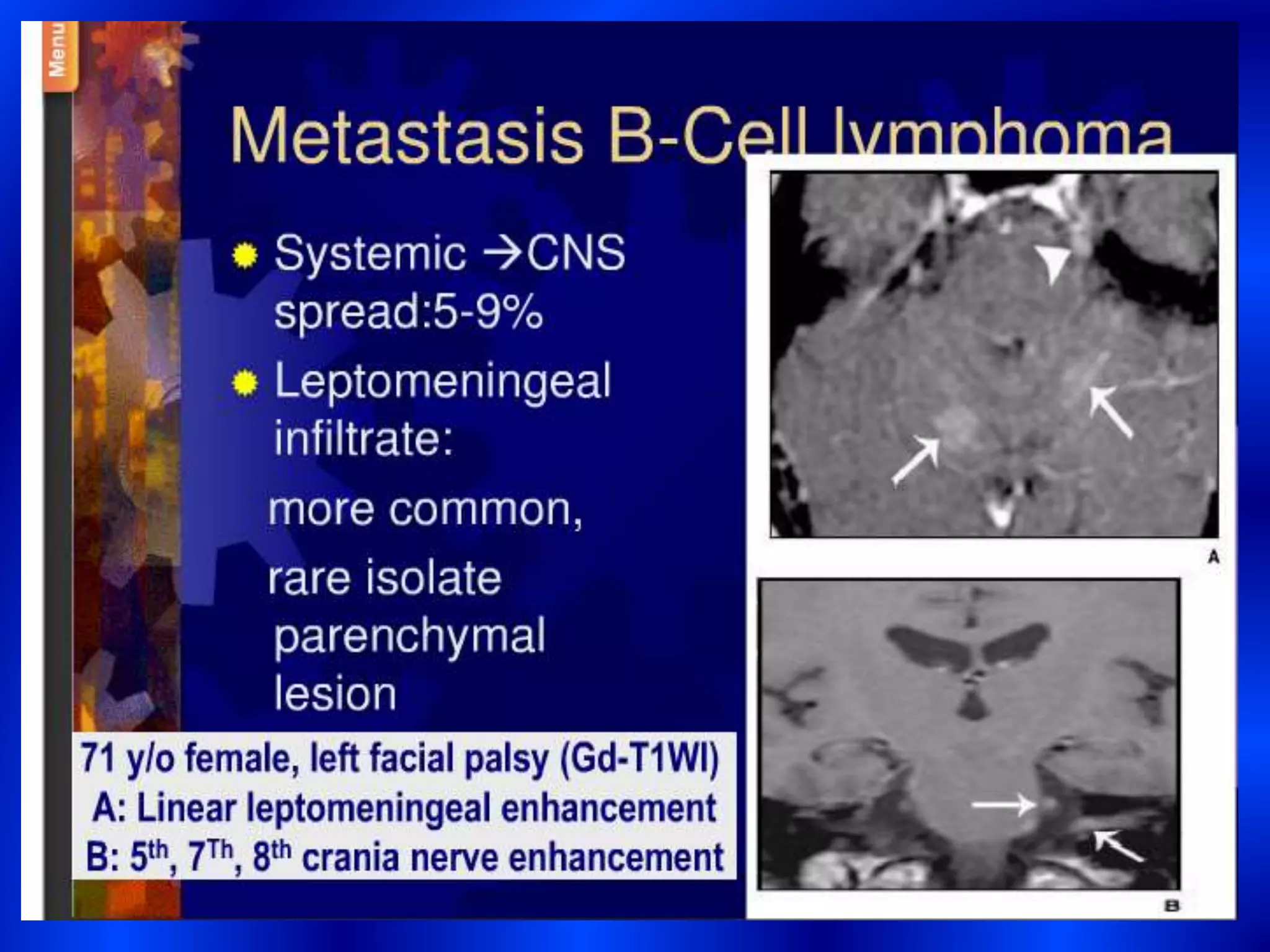
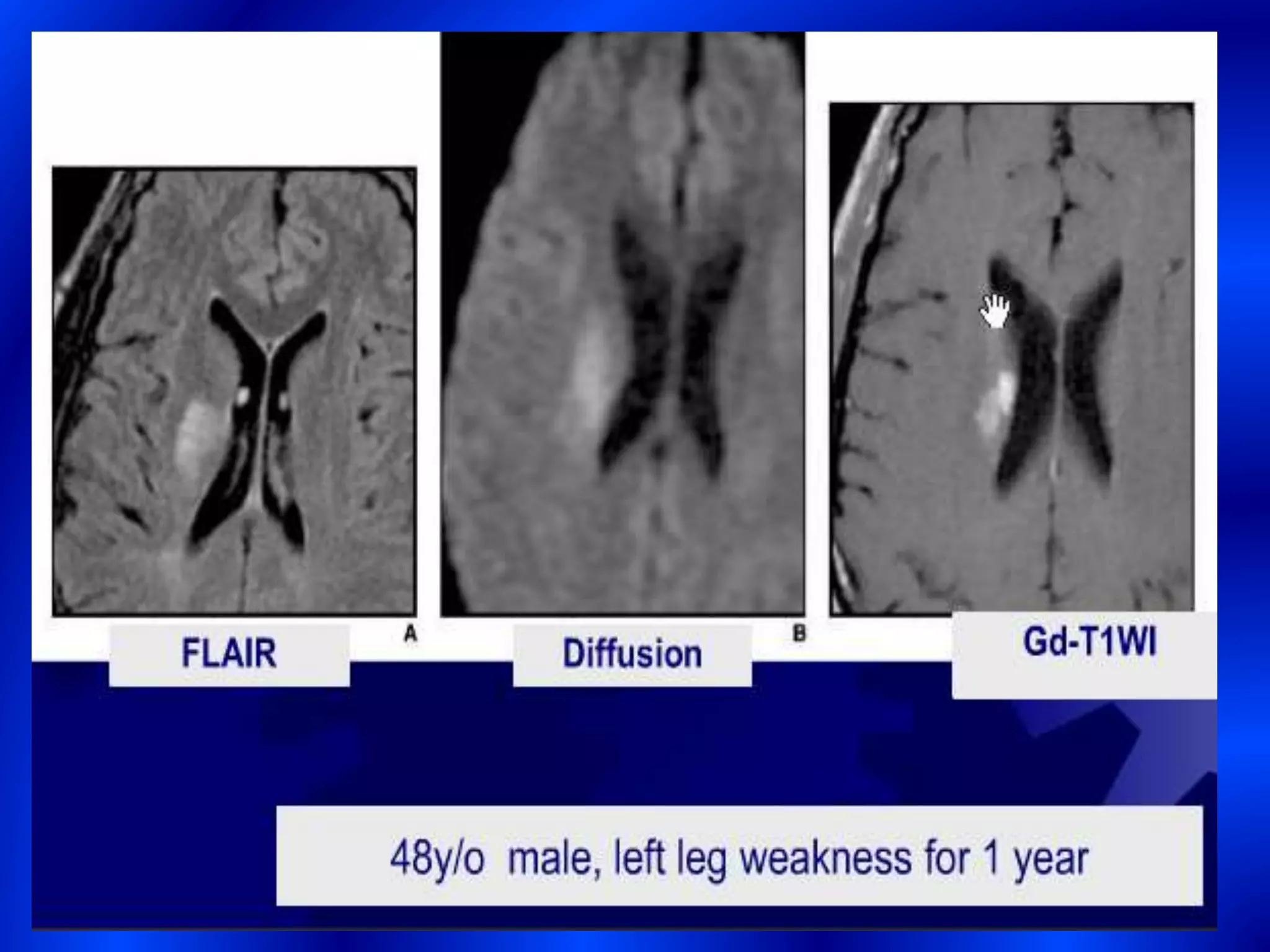
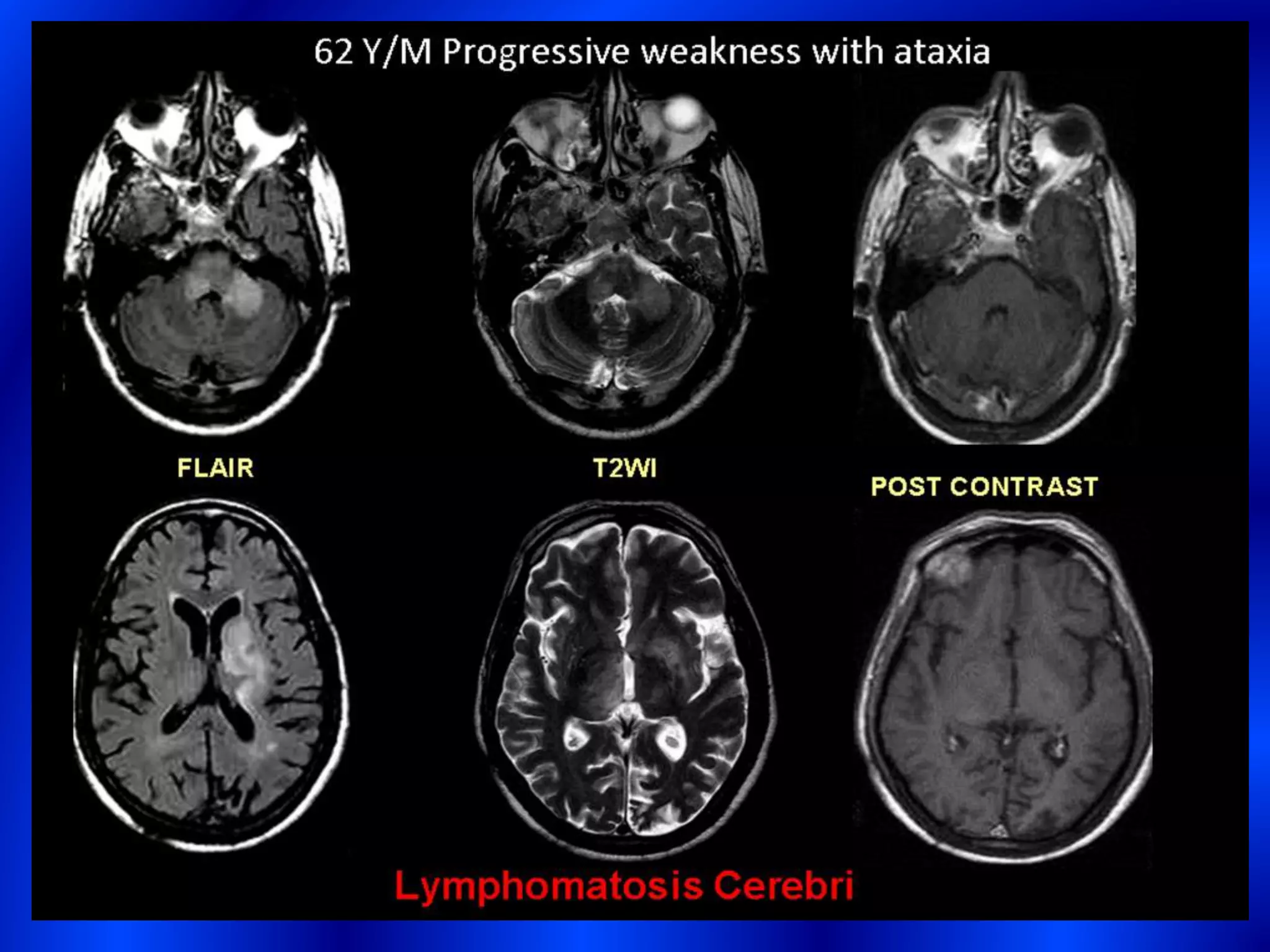
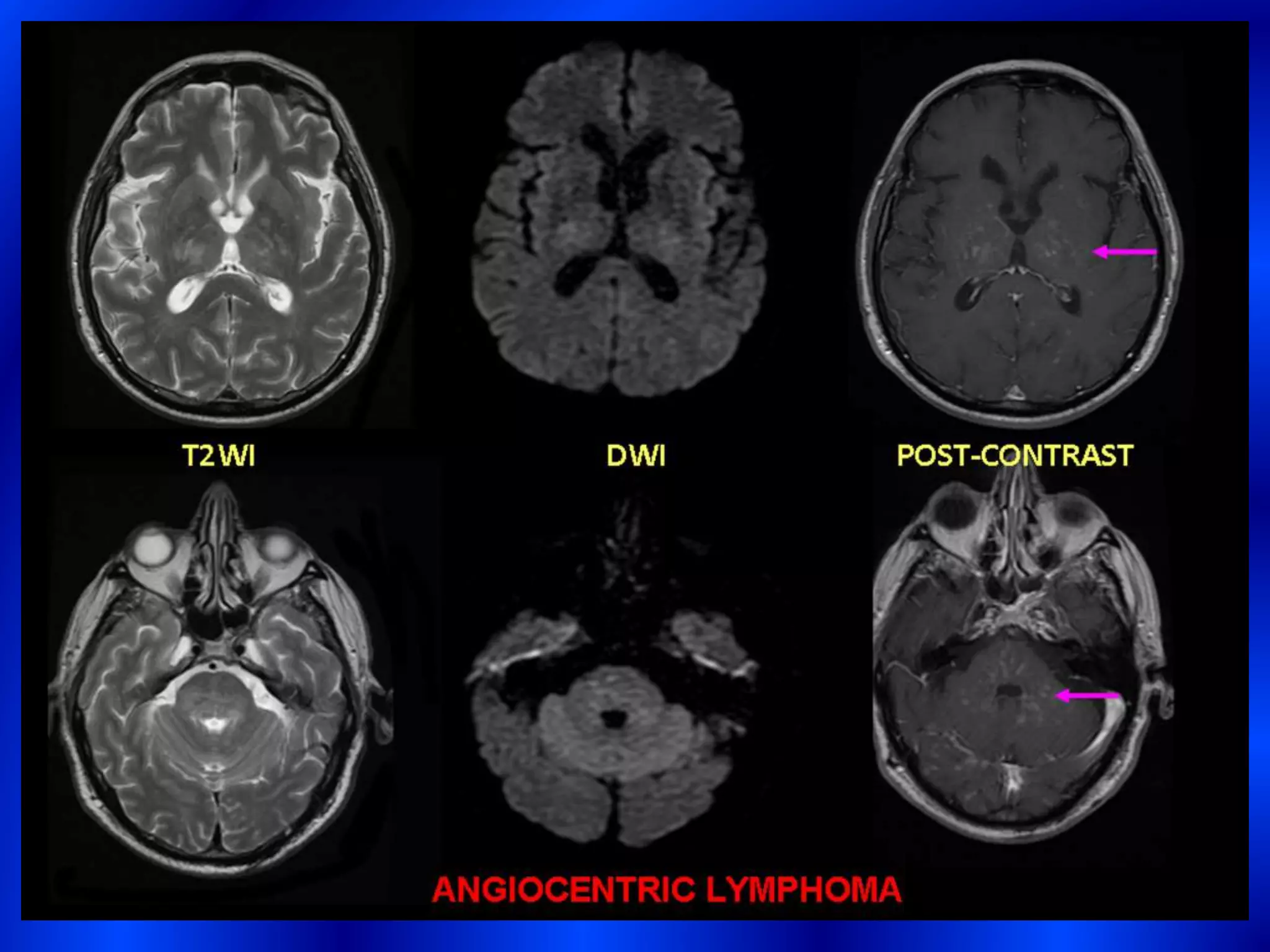
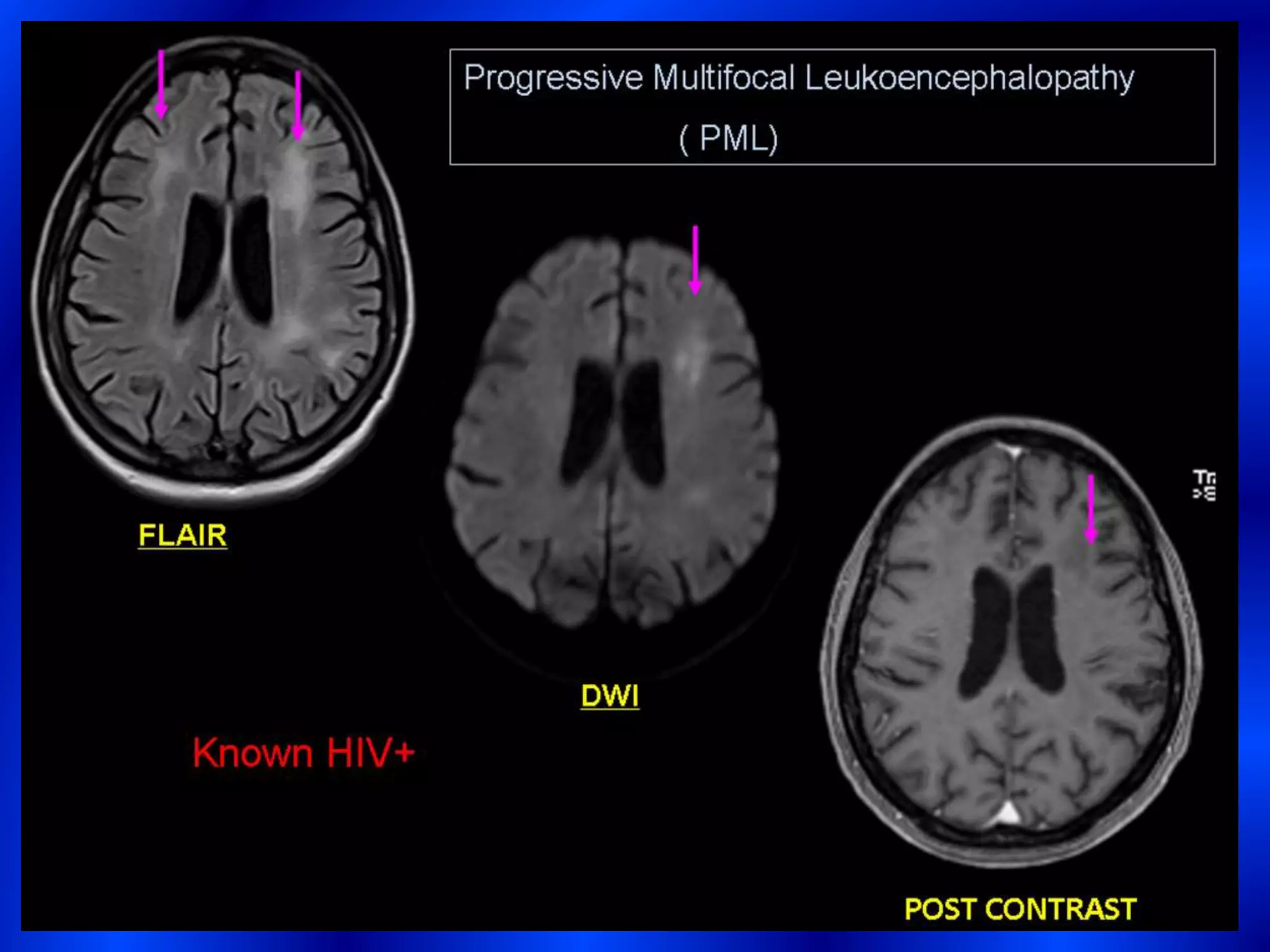
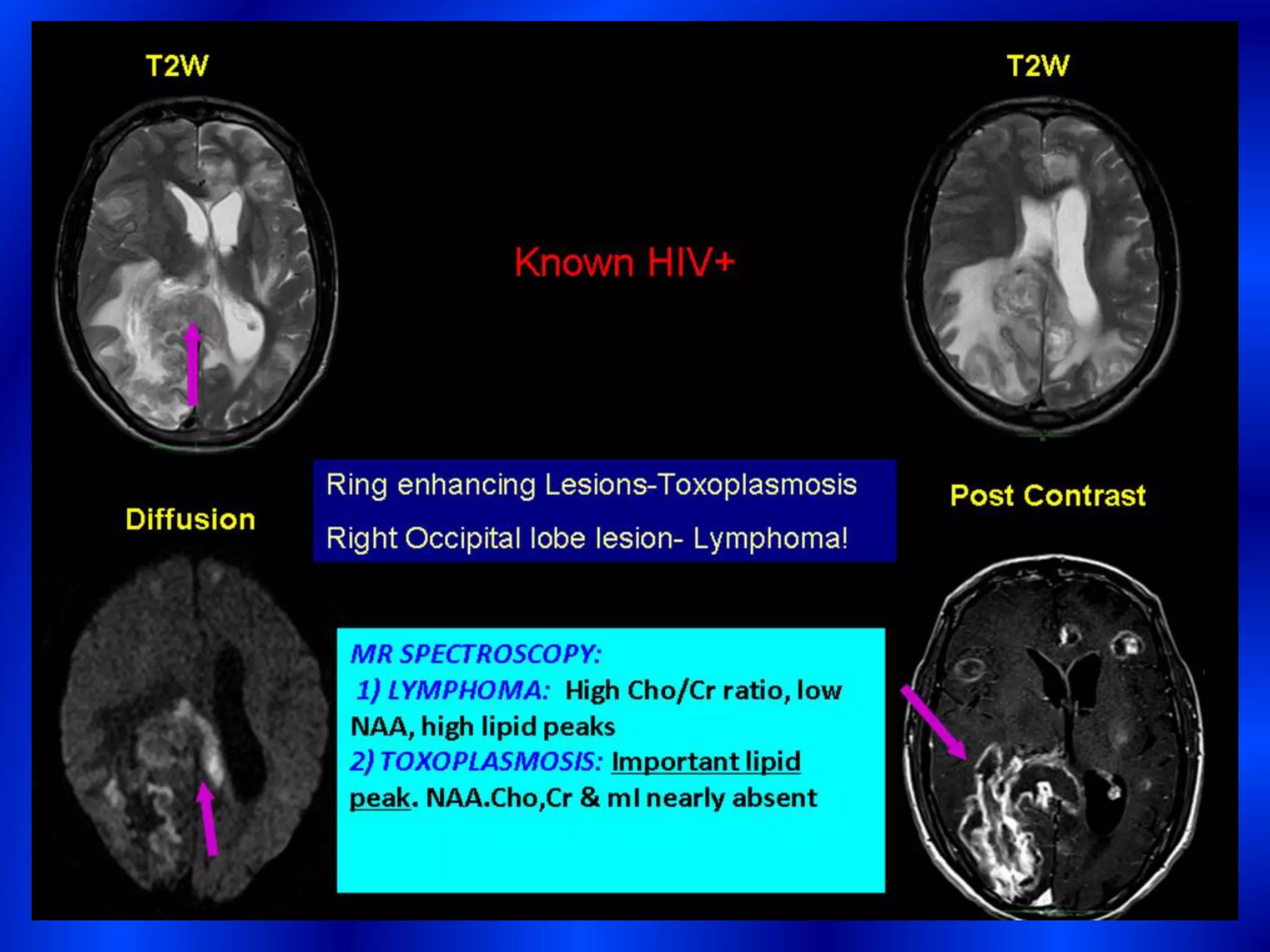


Primary central nervous system lymphoma (PCNSL) refers to lymphoma isolated to the brain and spinal cord. Imaging plays an important role in diagnosis. On CT, PCNSL typically appears as a hyperdense, solitary mass without necrosis or hemorrhage. On MRI, it has intermediate-low T1 signal, iso-hypointense T2 signal, and homogeneous enhancement. Location is commonly the supratentorial white matter. In immunocompromised patients, PCNSL can appear atypical with multiple lesions, necrosis, and heterogeneous enhancement. Advanced techniques like perfusion MRI and PET can aid in differentiating PCNSL from other tumors like glioblastoma and metastasis.











































































































