Downloaded 453 times
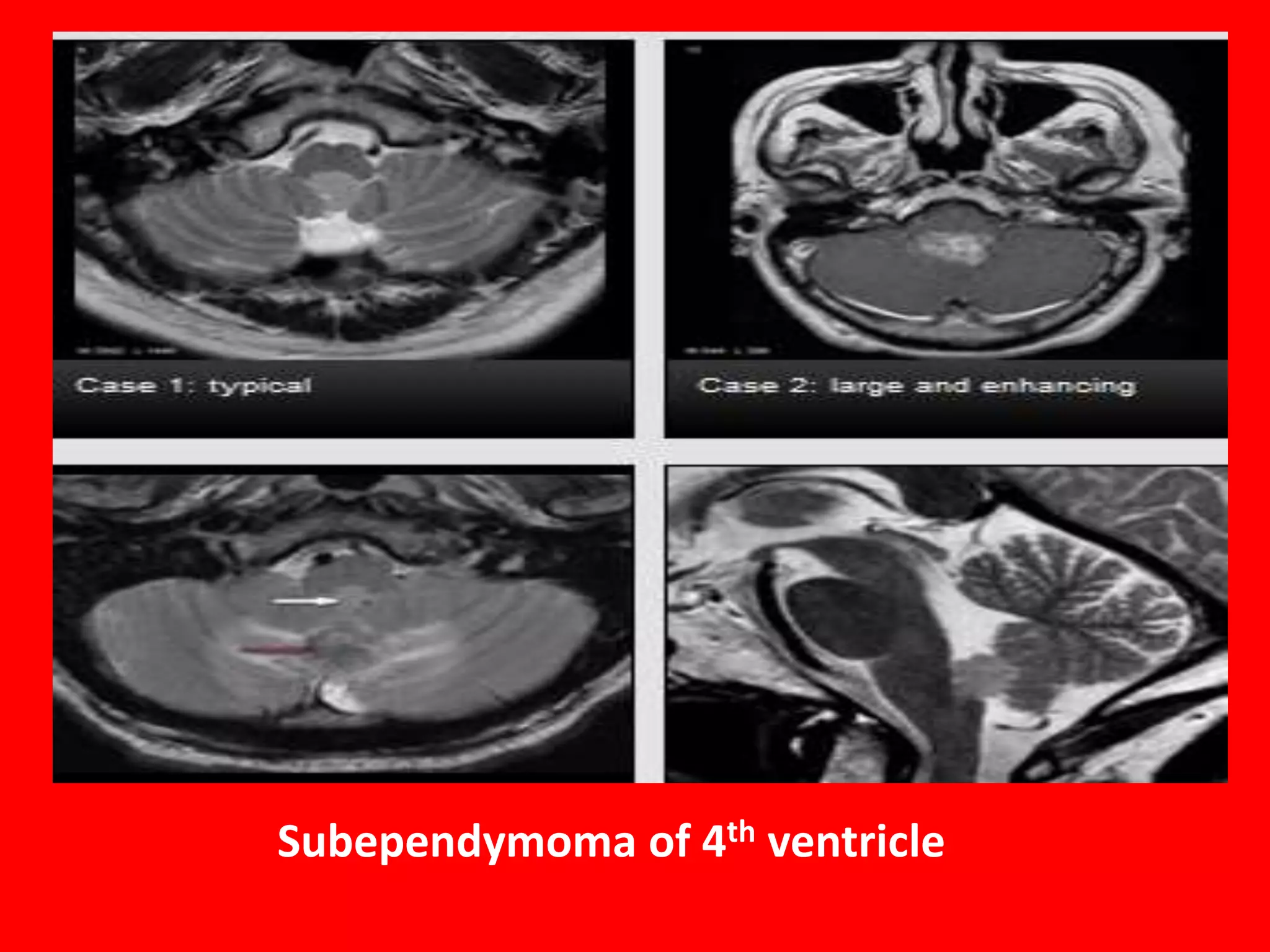
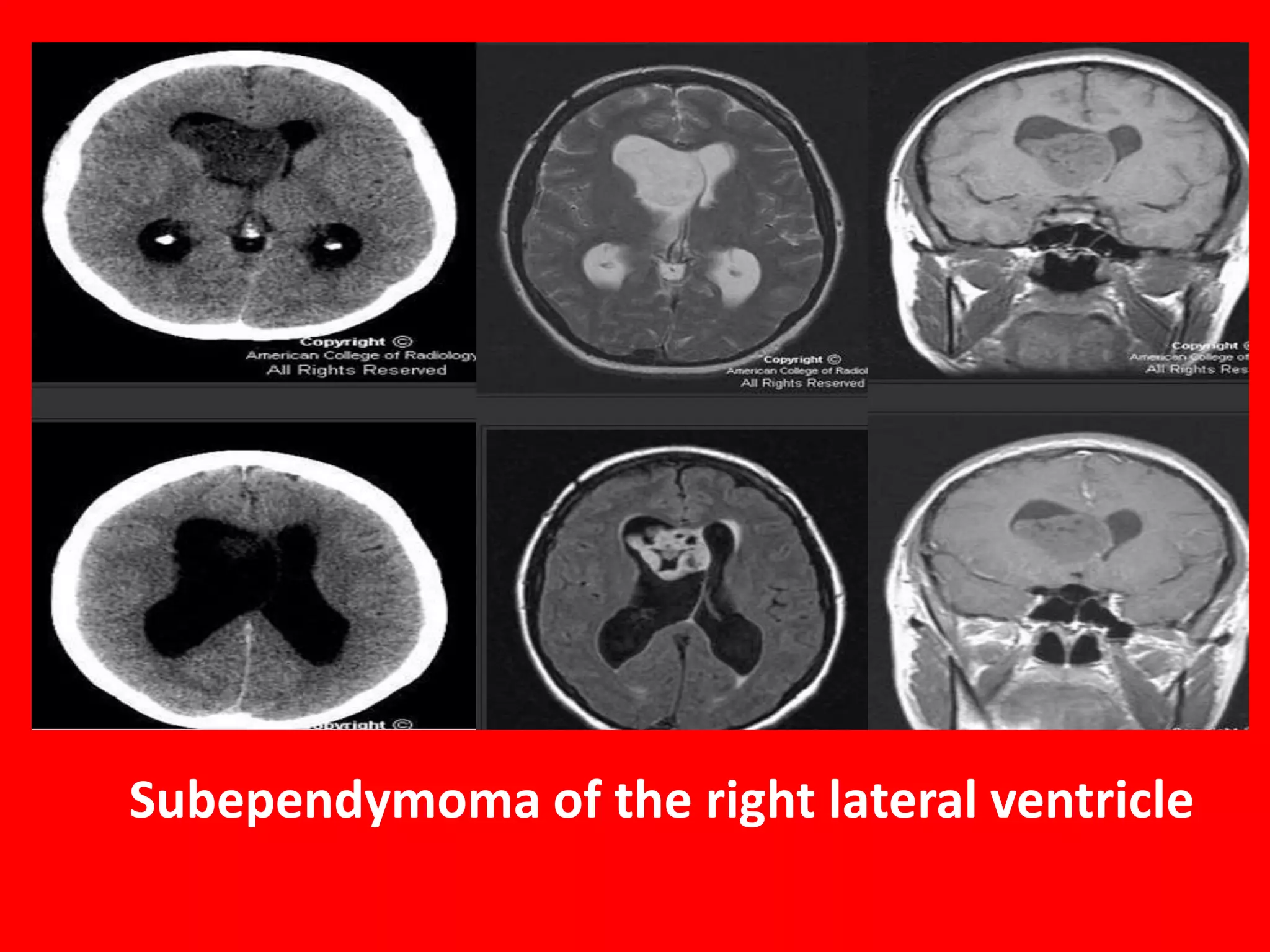
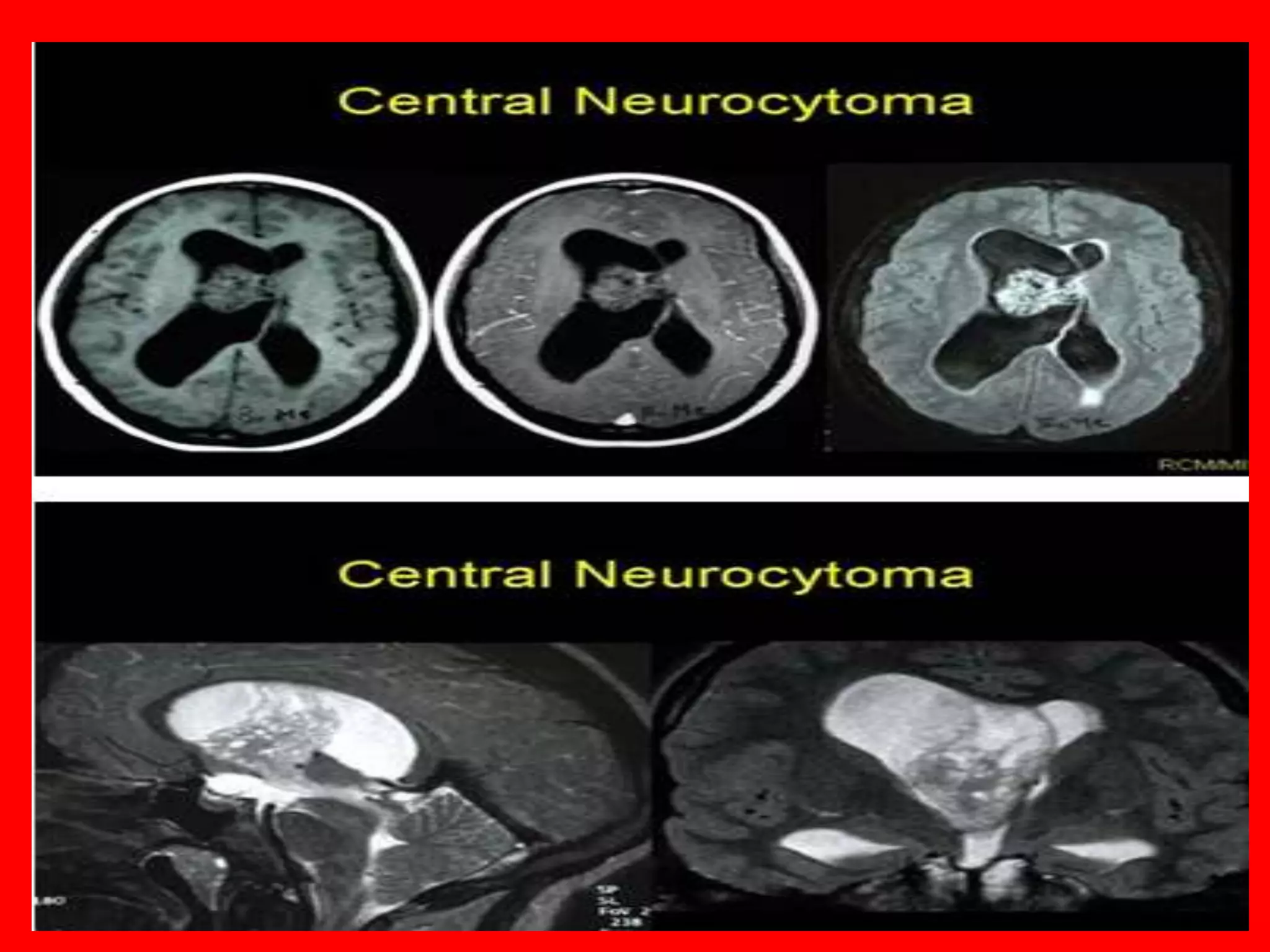
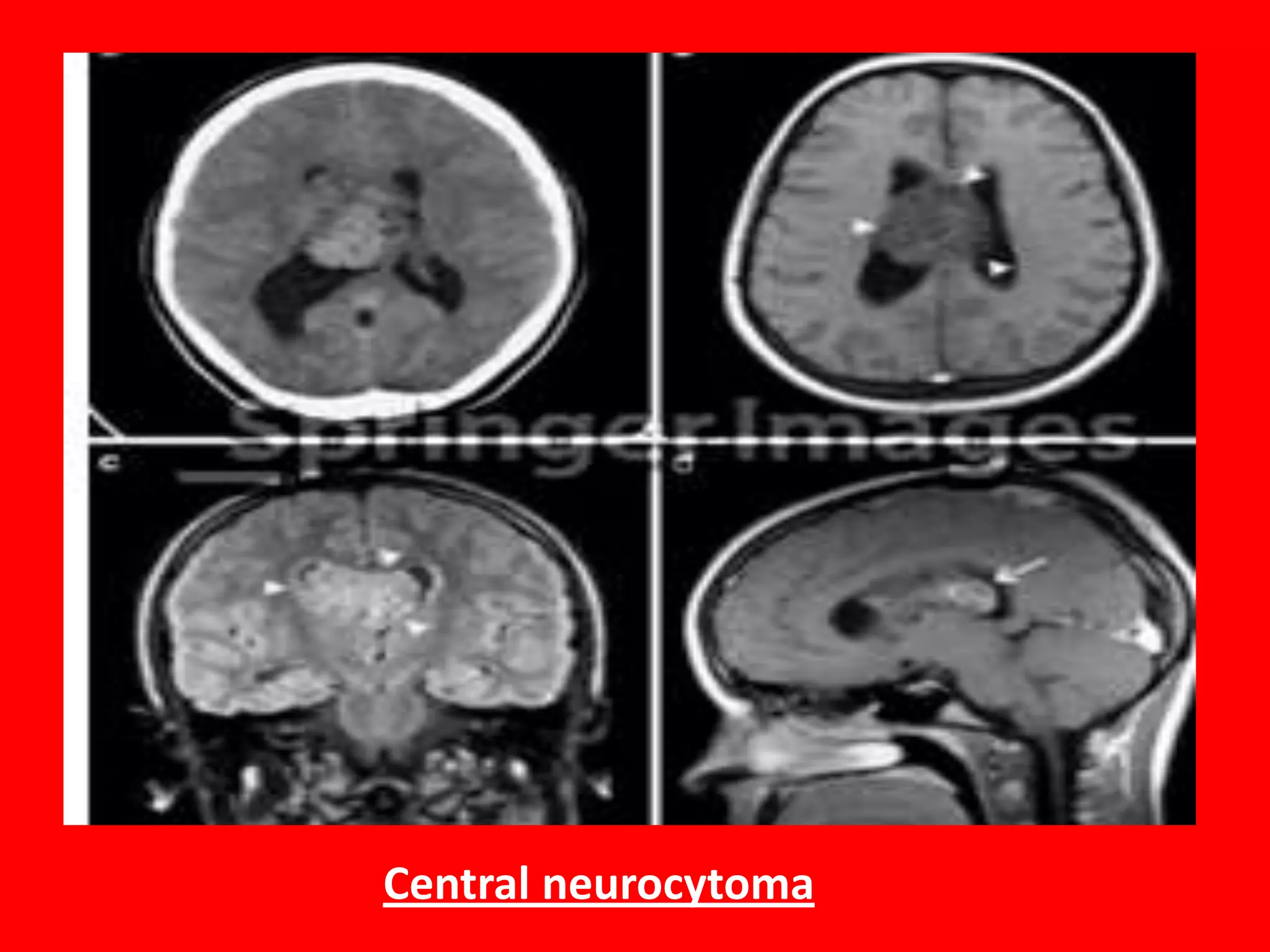
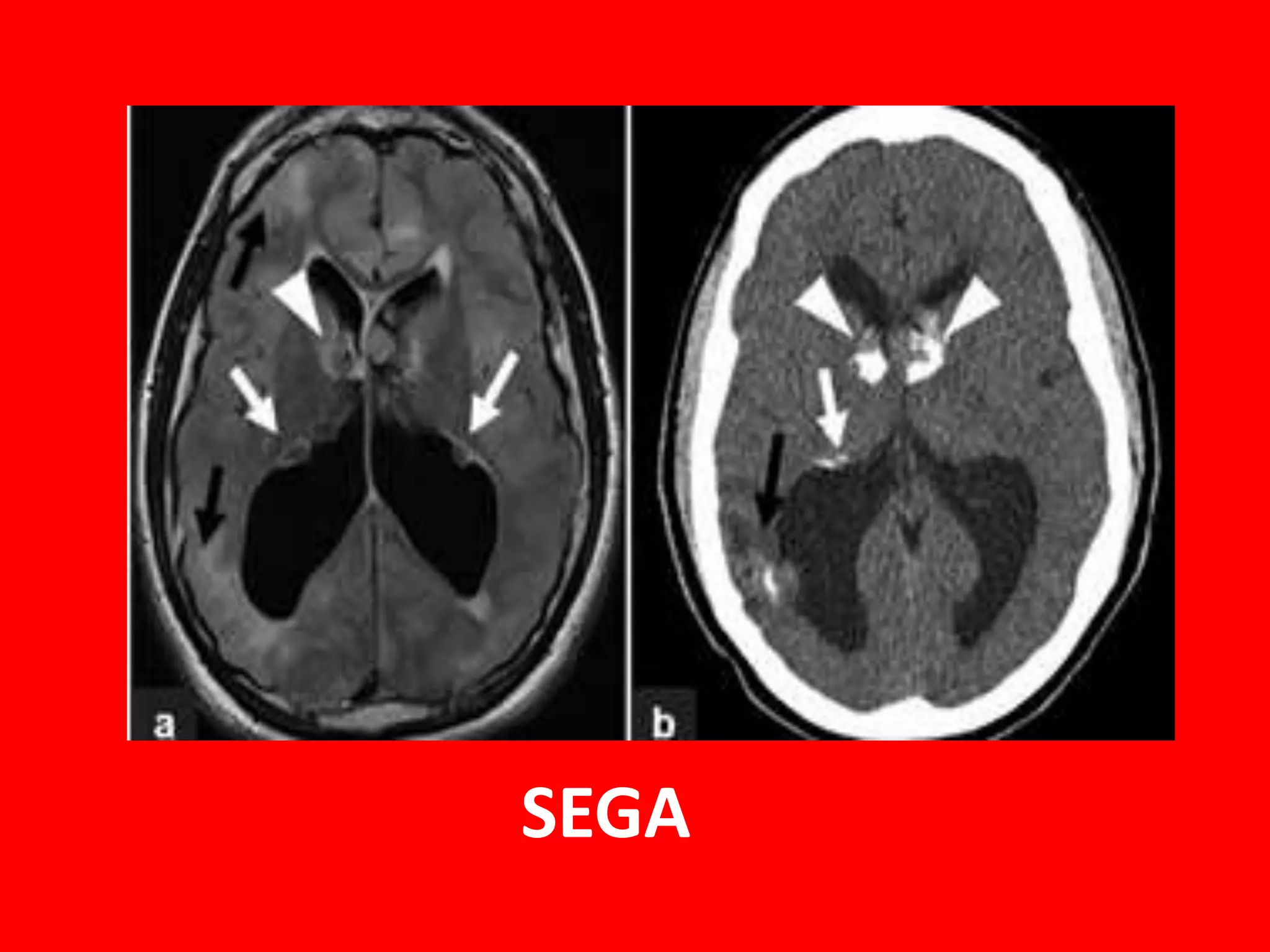
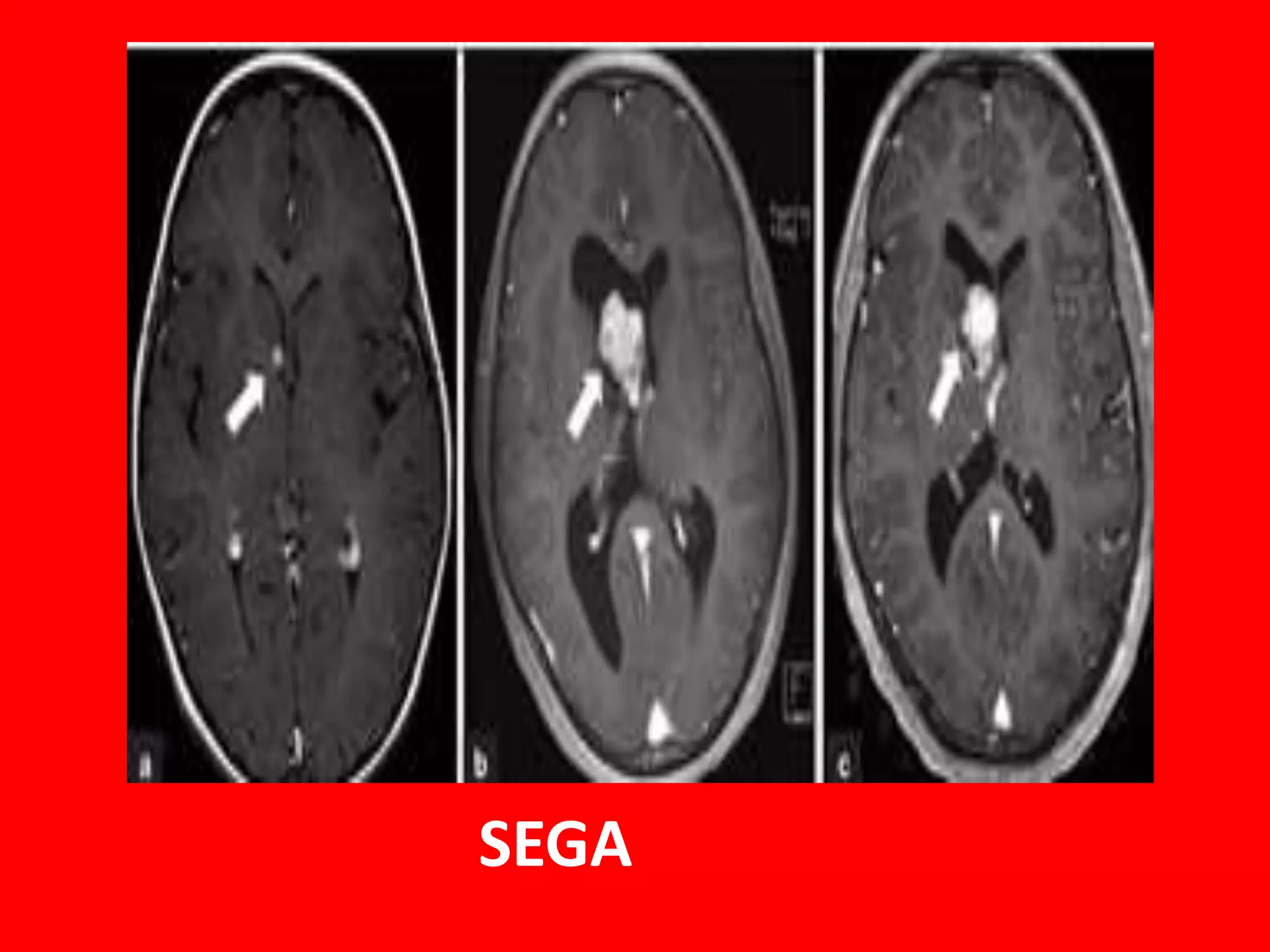
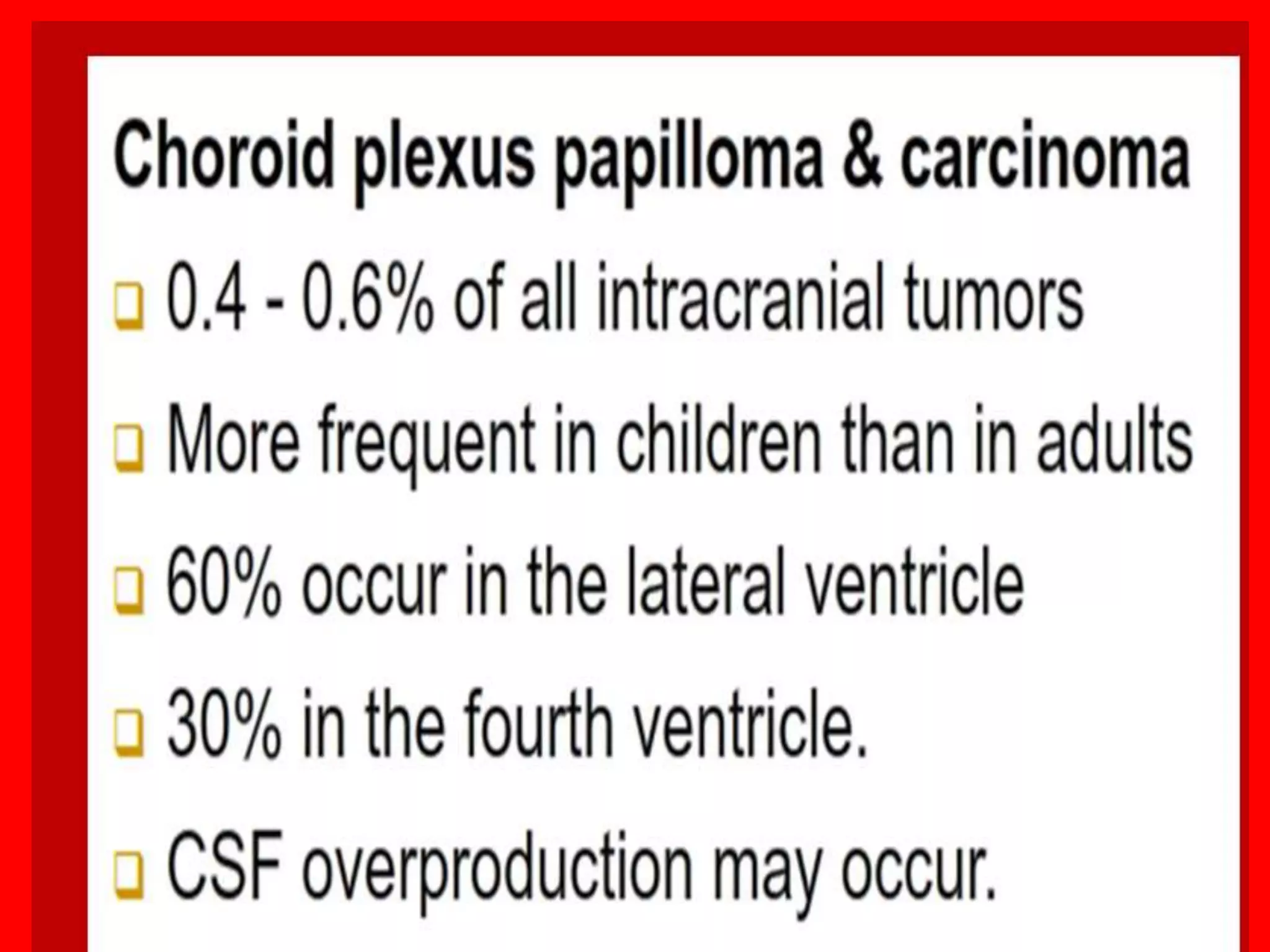
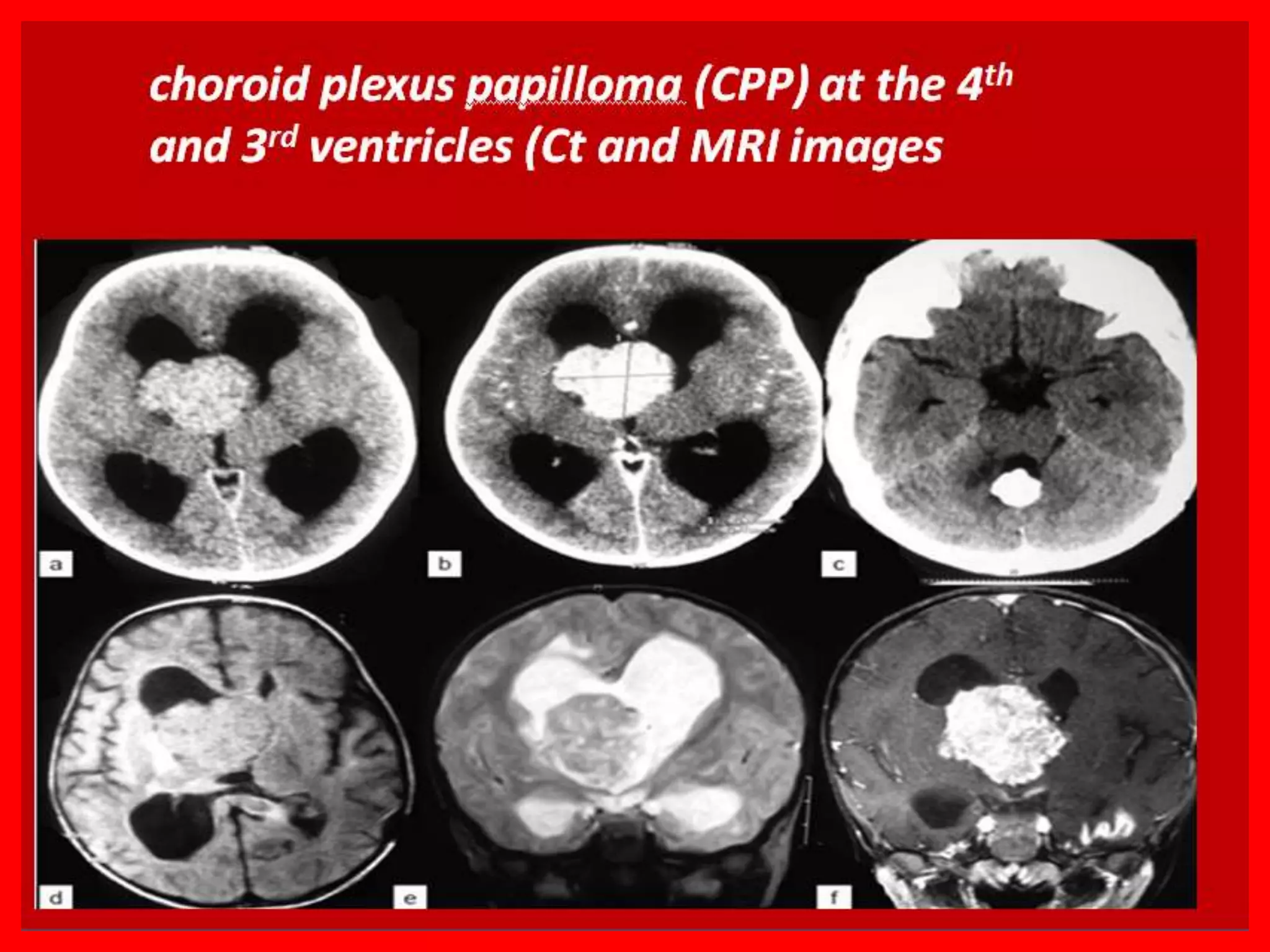
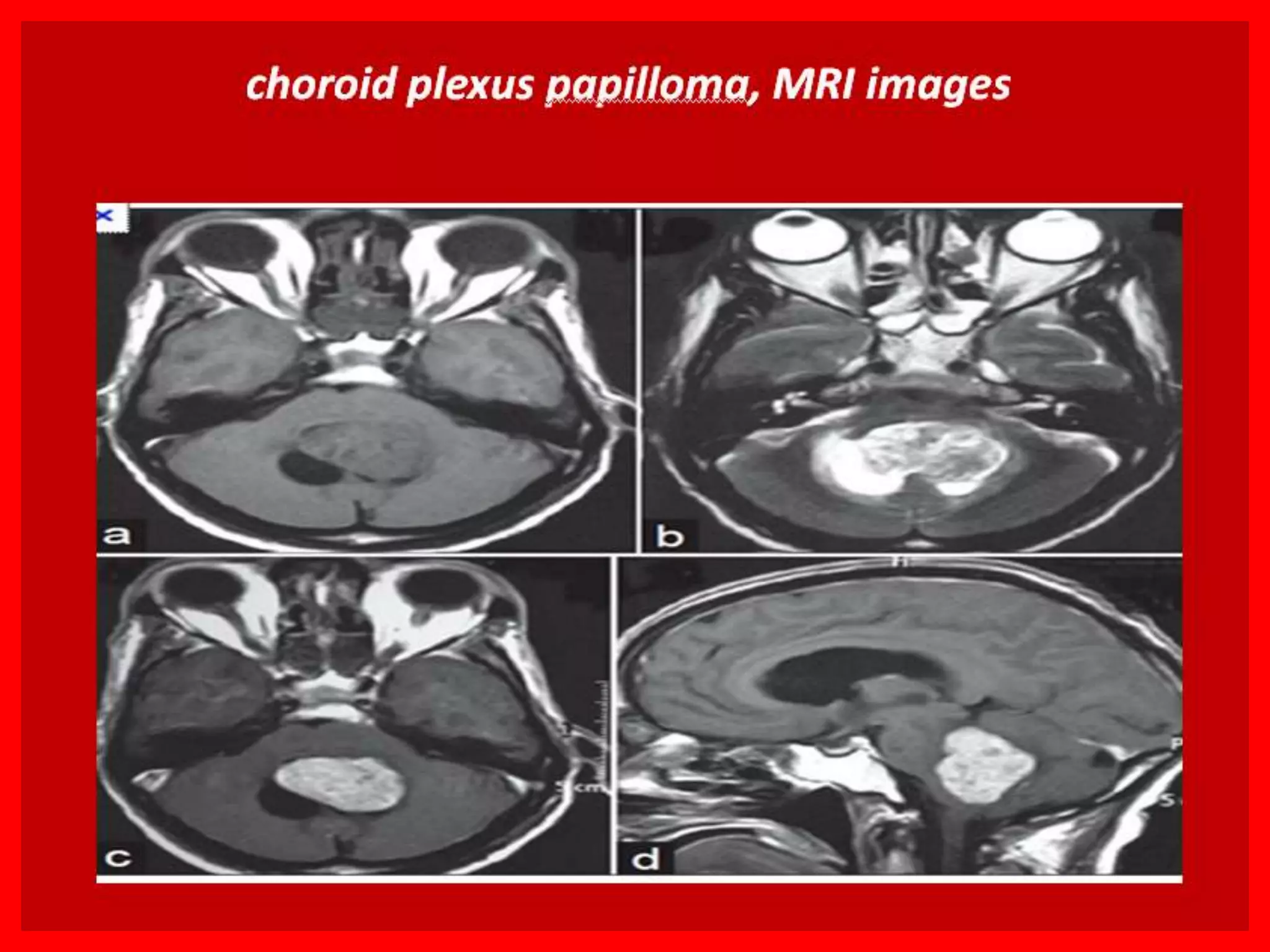
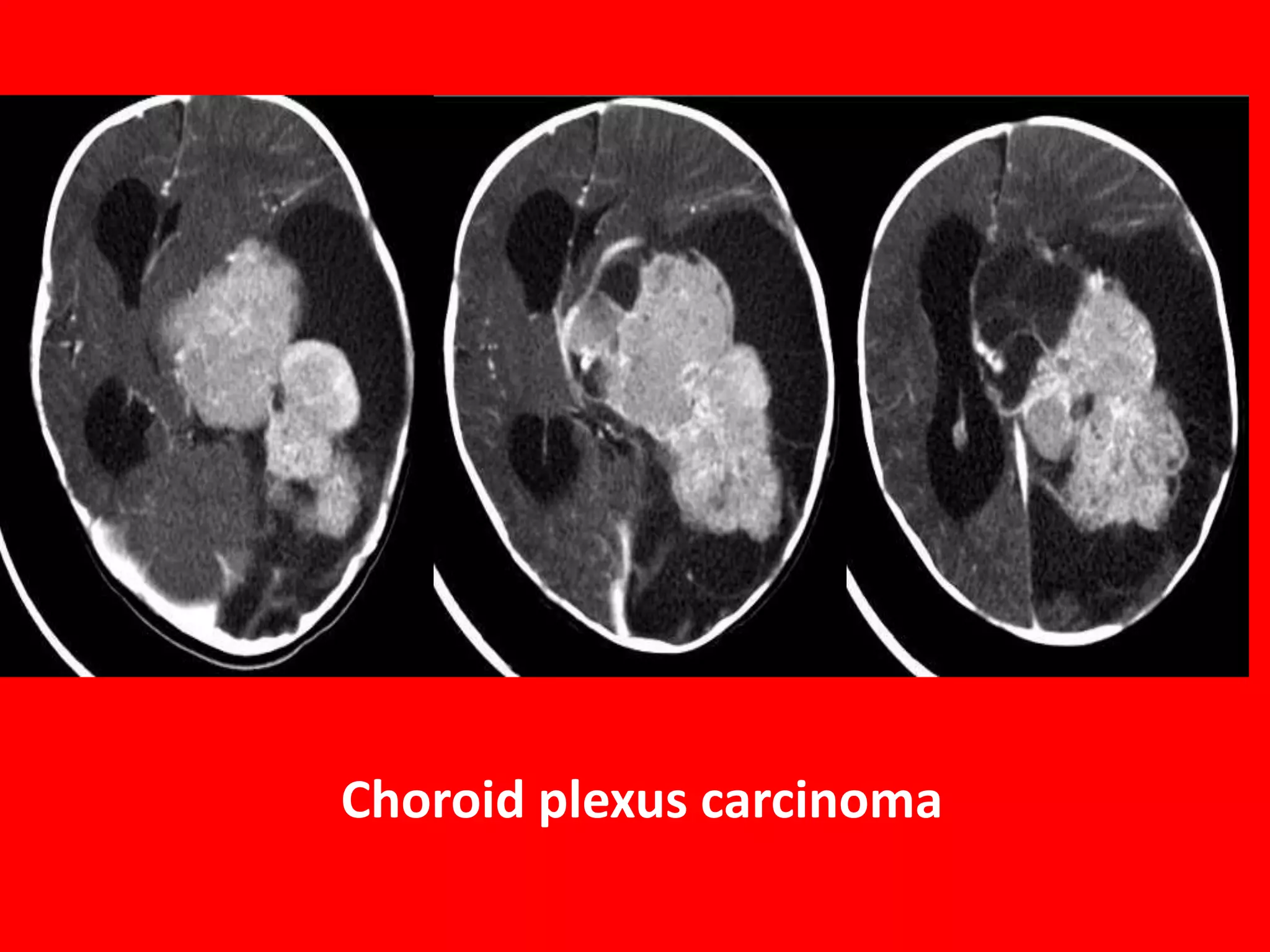
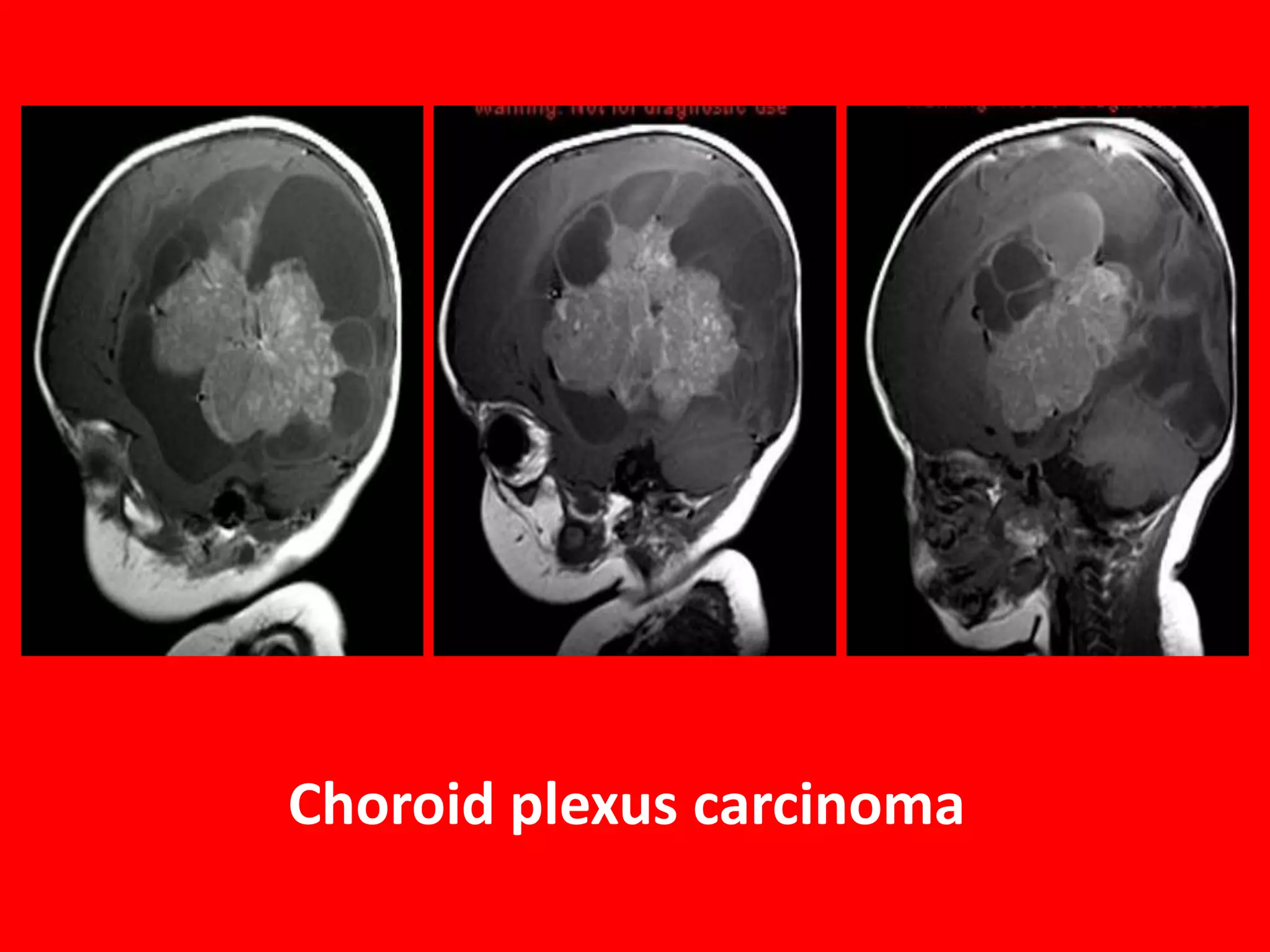
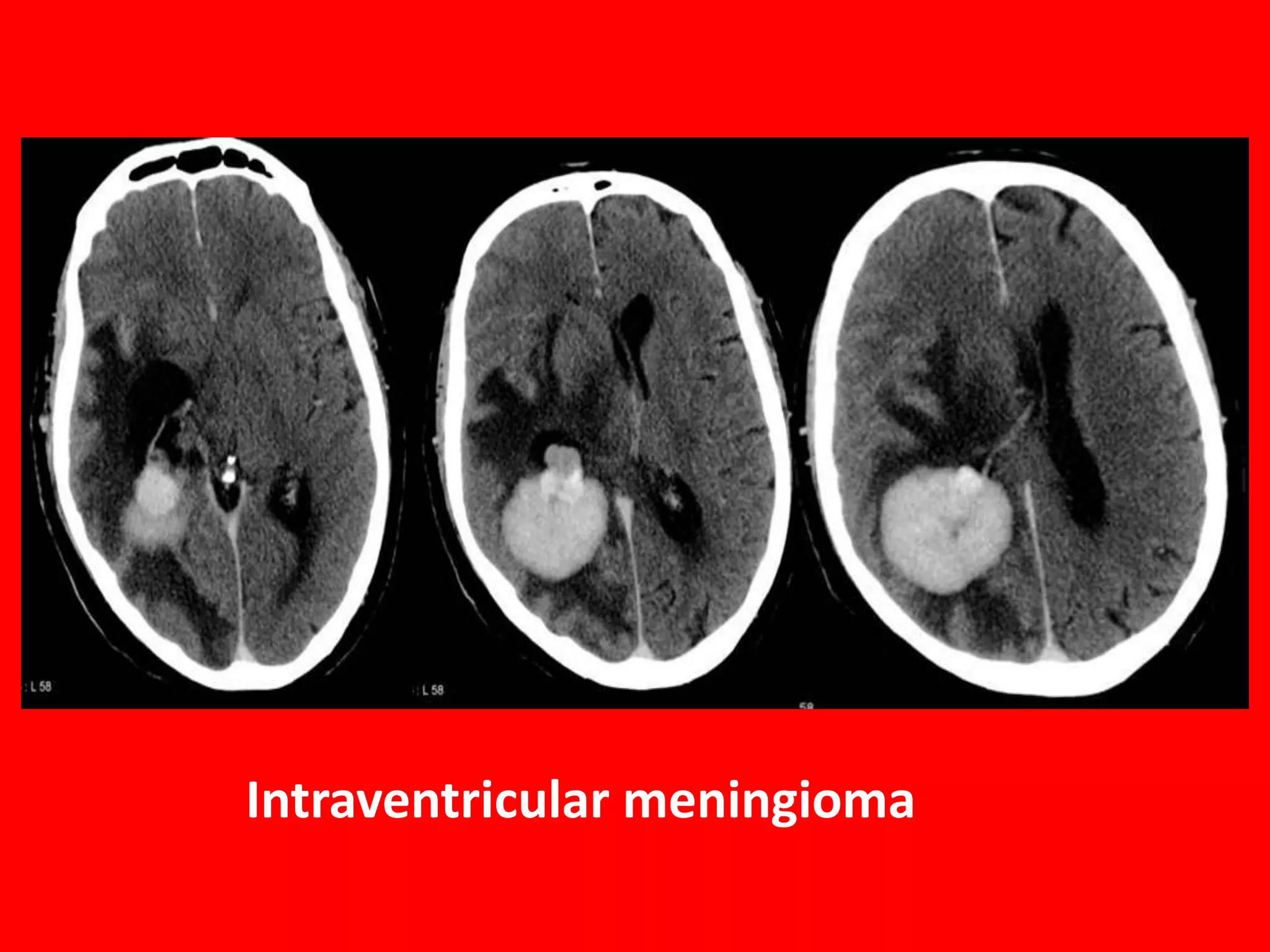
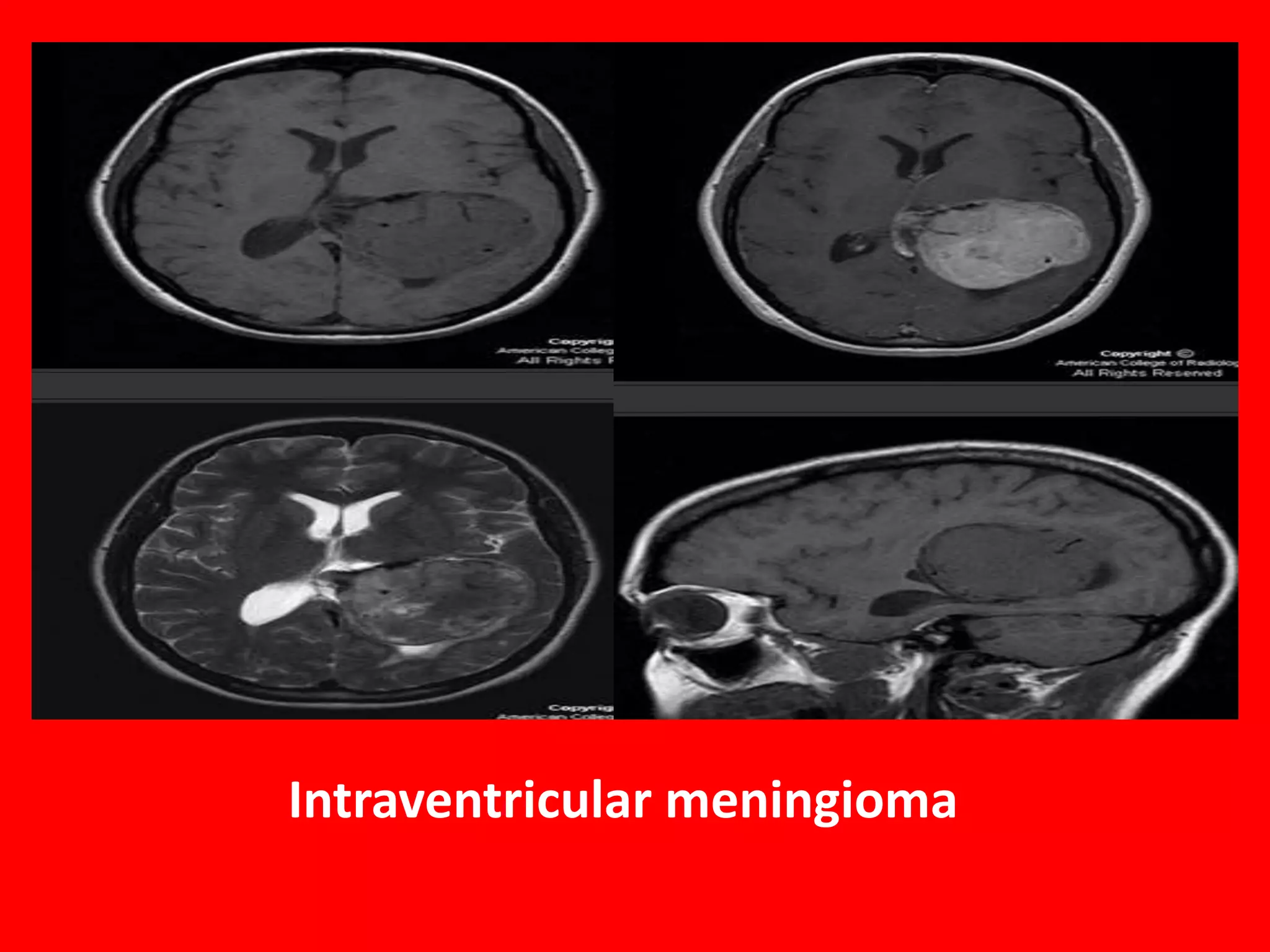
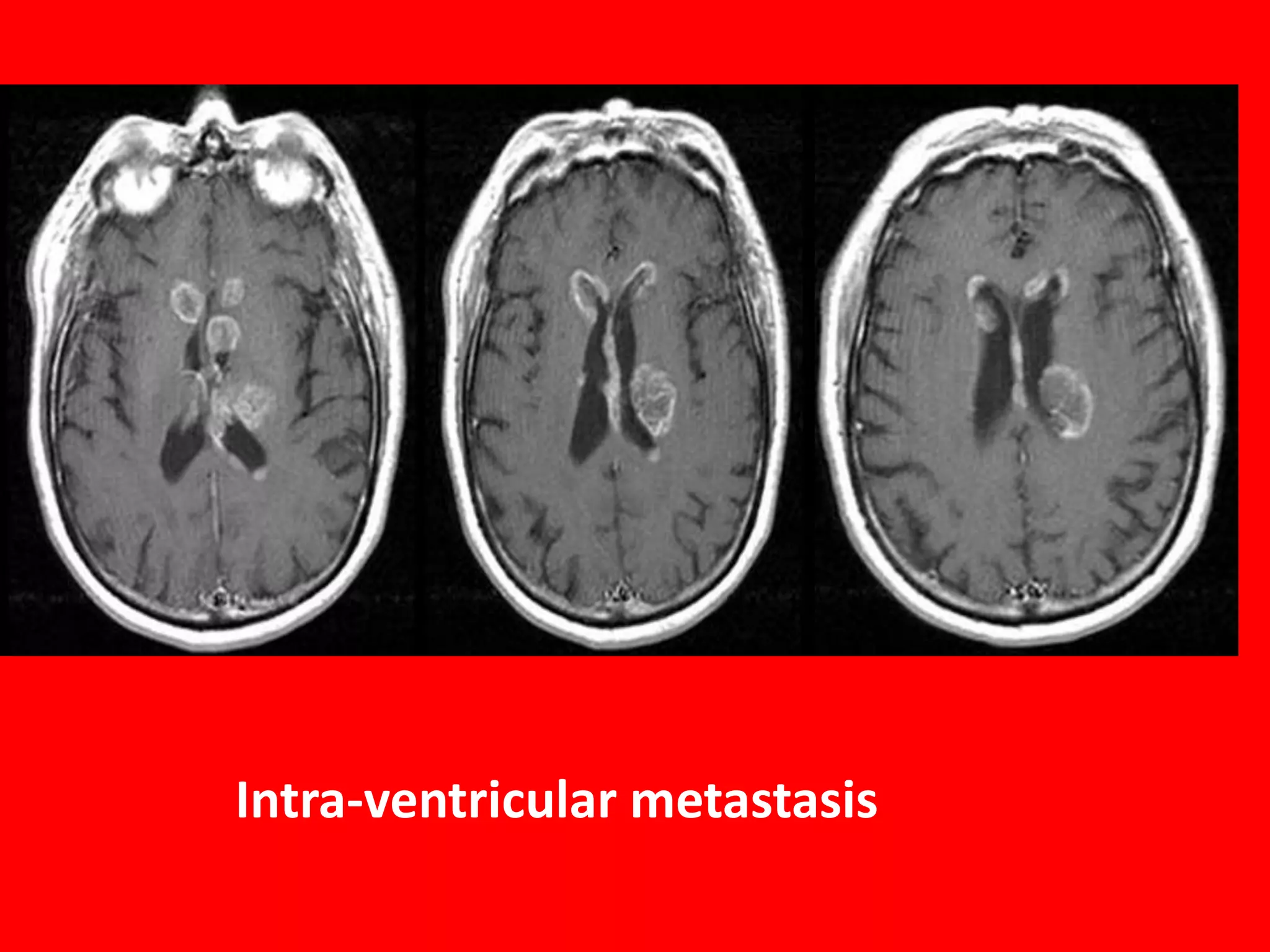
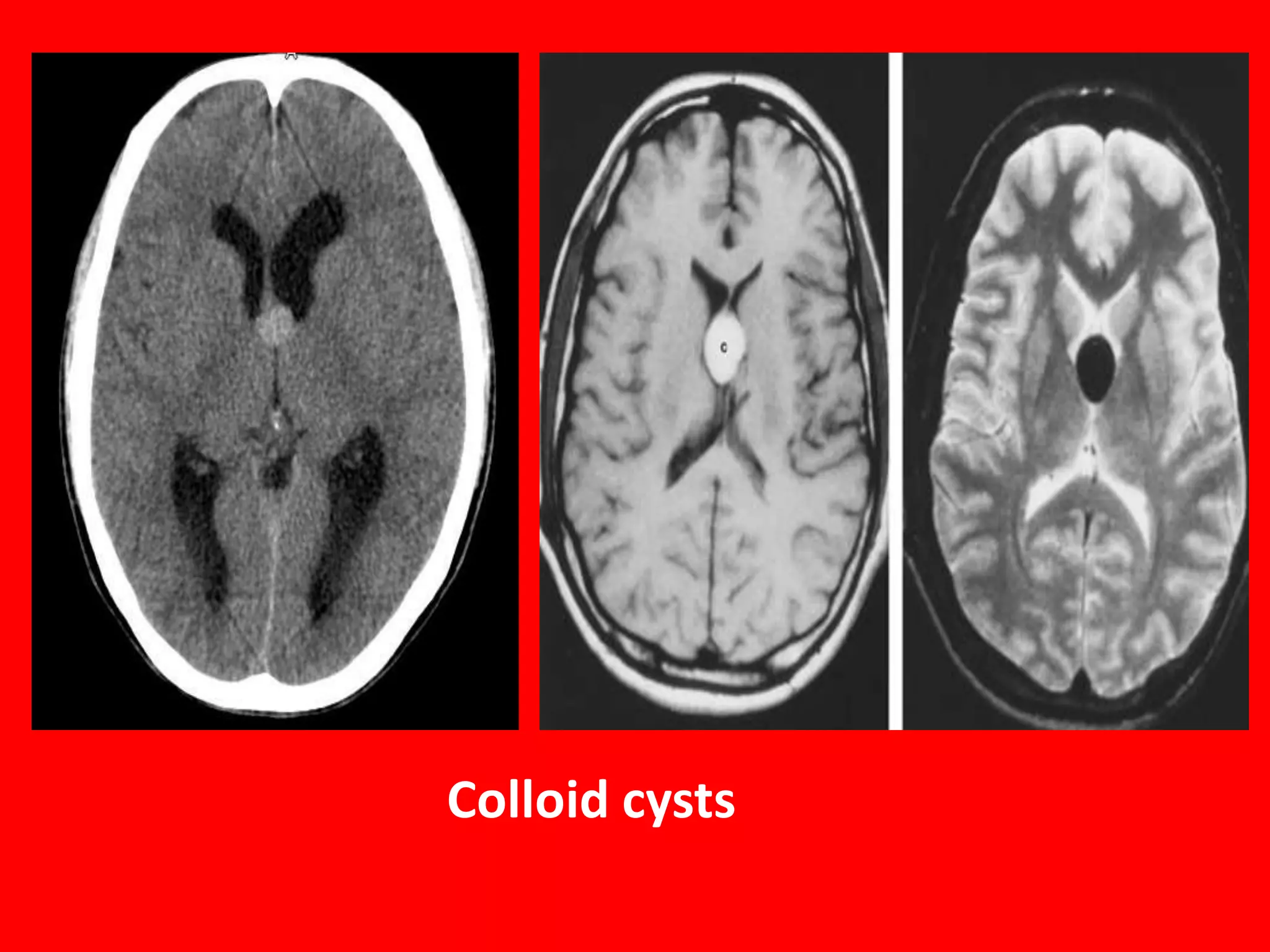
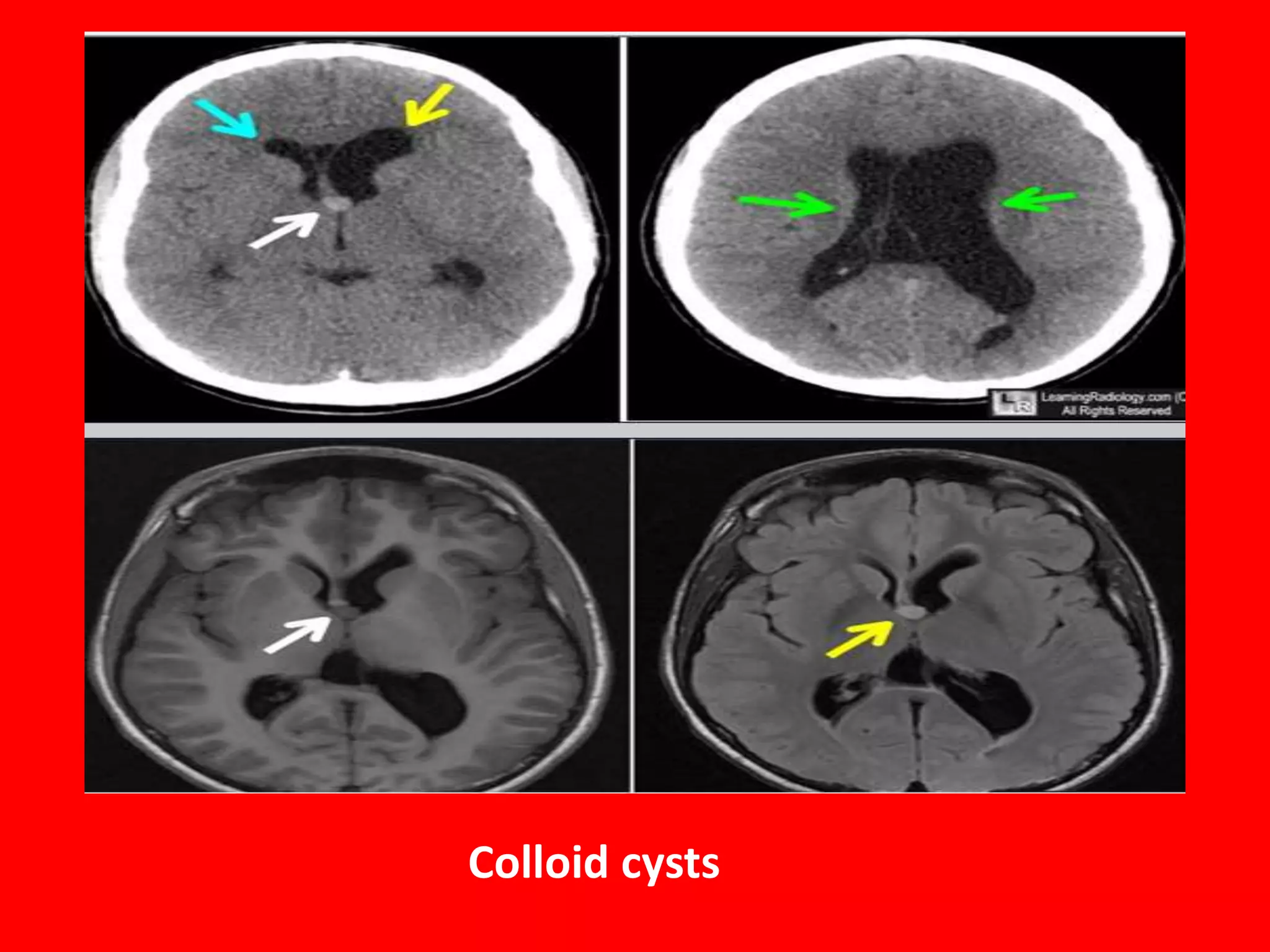
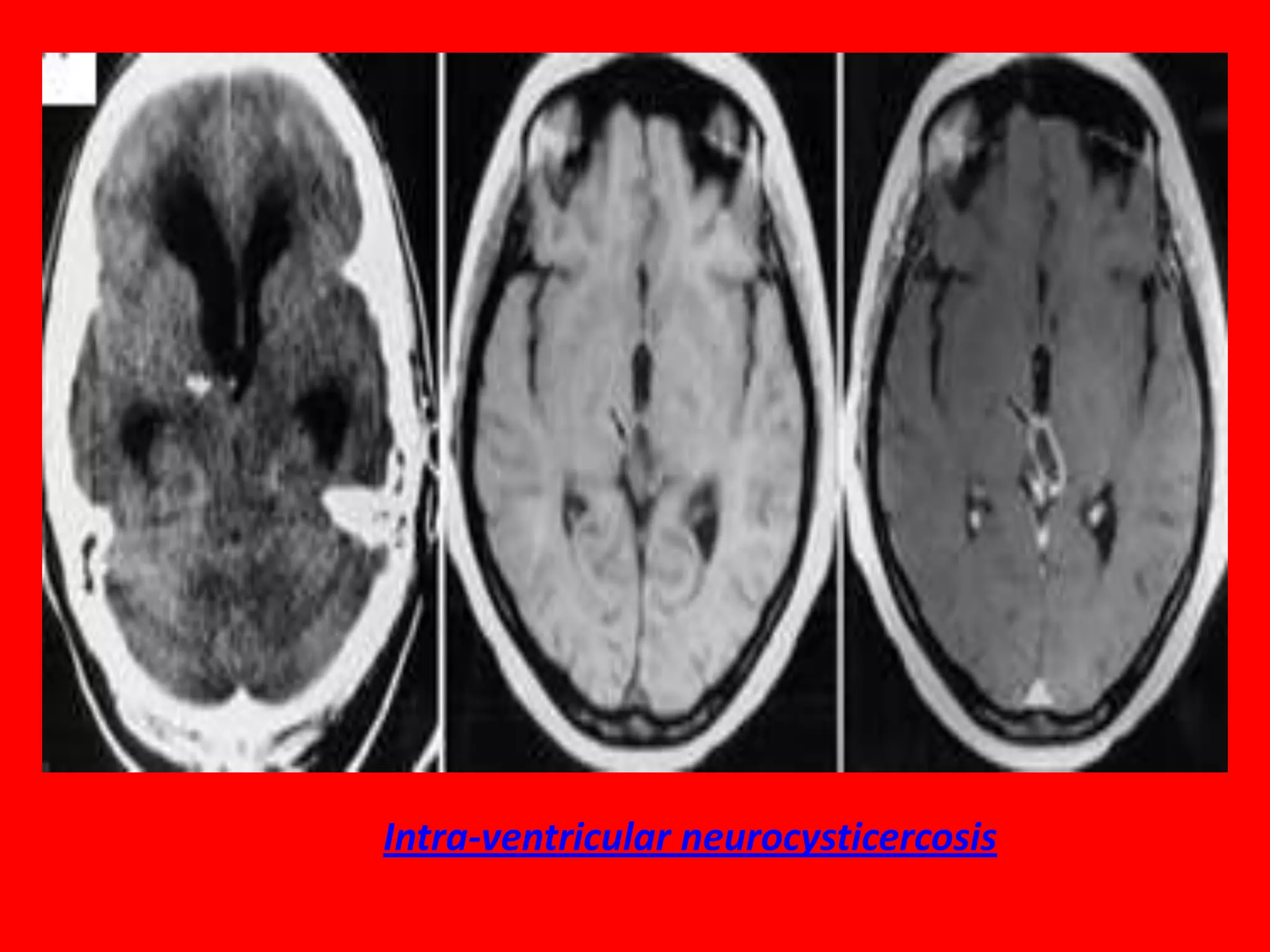
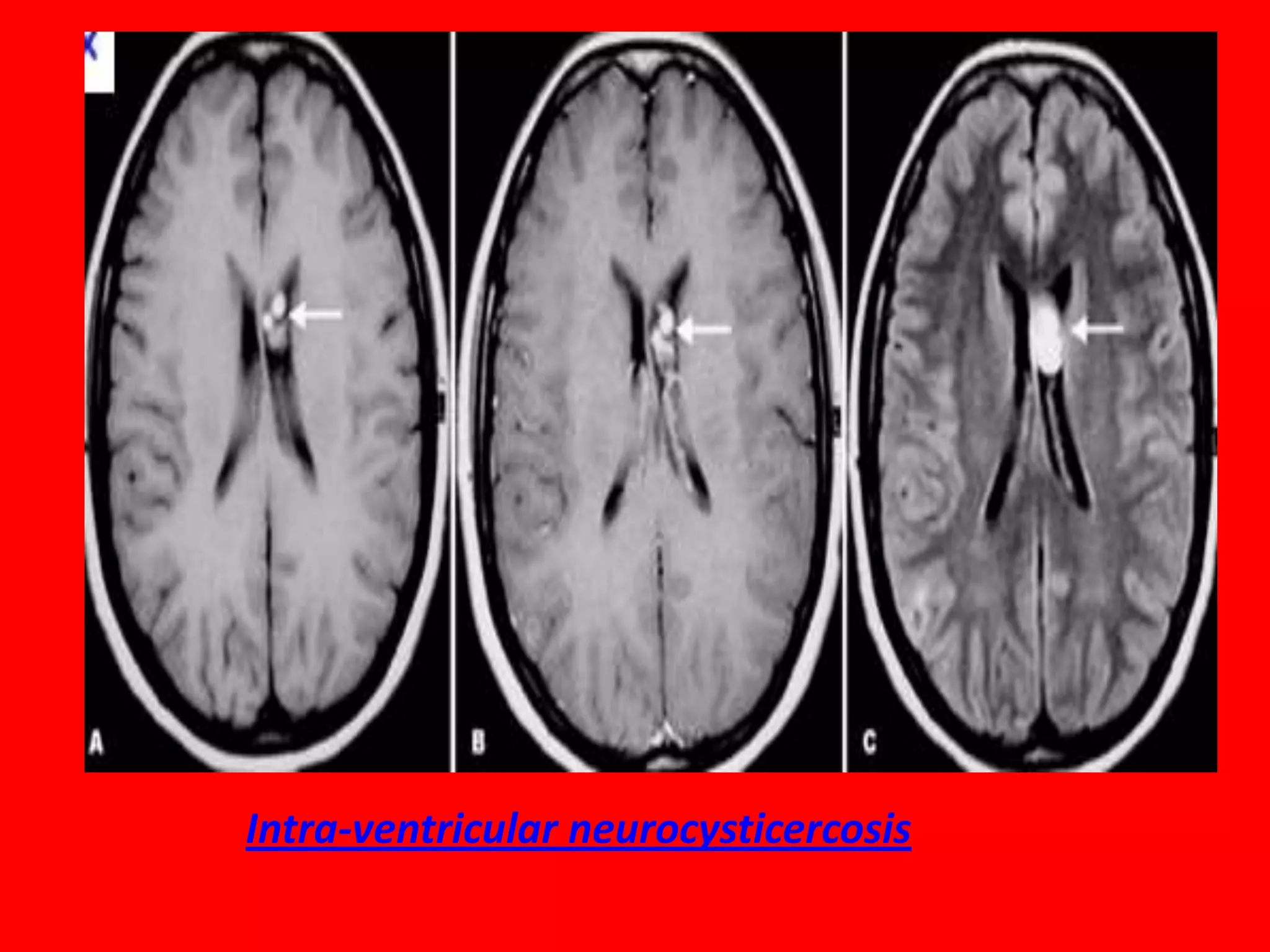
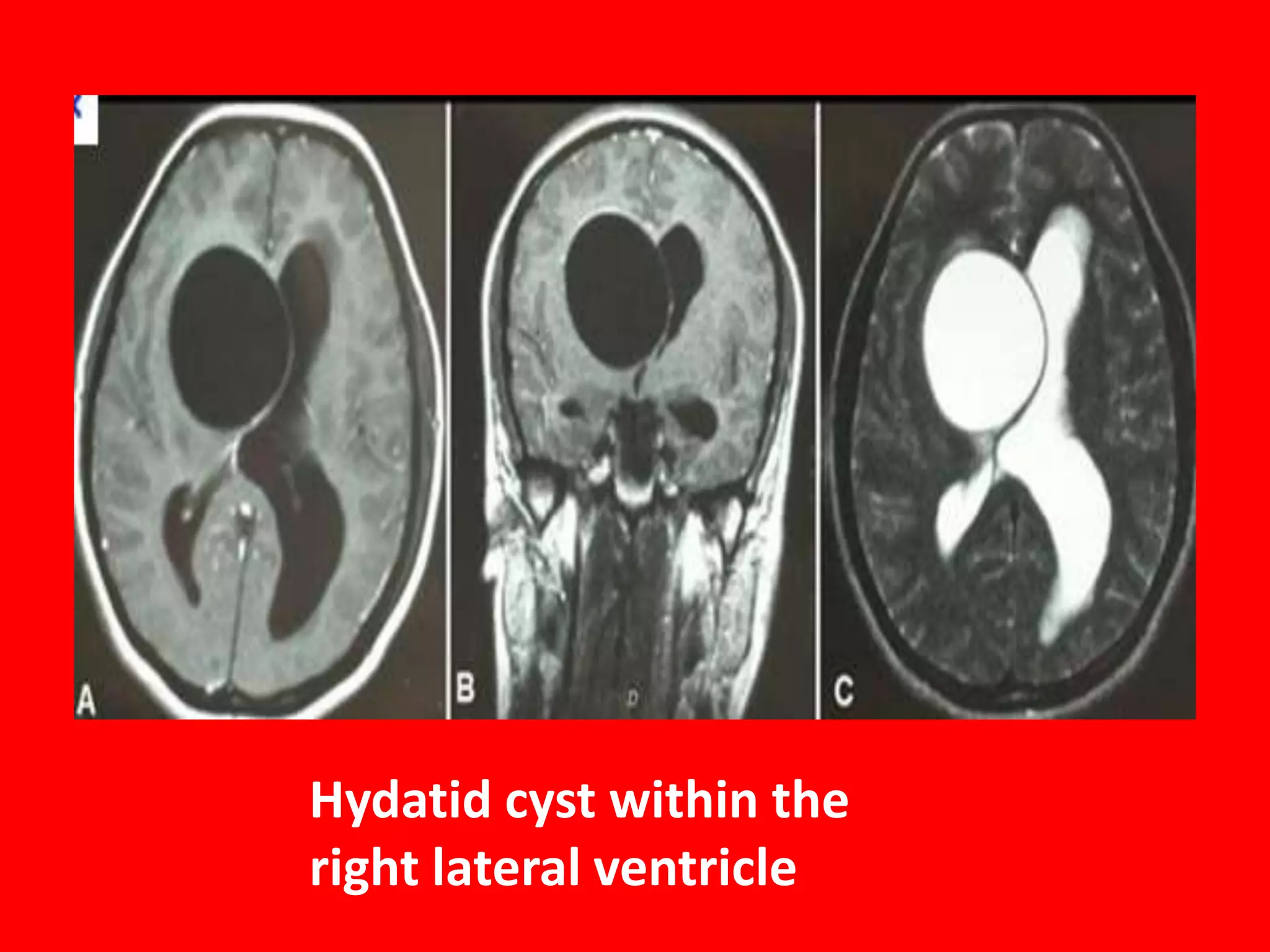


This document discusses various types of intraventricular tumors and other lesions. It describes tumors that originate from the ventricular walls, septum pellucidum, and choroid plexus, including ependymoma, subependymoma, central neurocytoma, subependymal giant cell astrocytoma, choroid plexus papilloma, choroid plexus carcinoma, and meningioma. It also discusses other intraventricular lesions like metastasis, colloid cysts, neurocysticercosis, hydatid cyst, and tuberculoma. Specific examples are provided with images of subependymoma, central neurocytoma, subependymal giant cell astro























































































