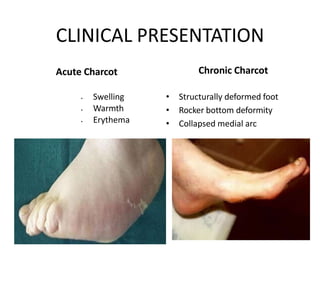
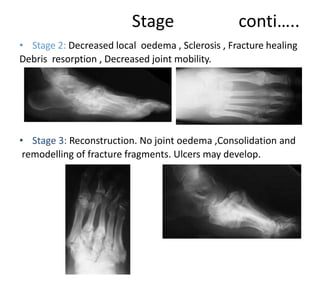
This document provides information about Charcot disease (neuropathic osteoarthropathy). It begins with a brief history, noting early descriptions by Musgrave and Charcot. Charcot disease is defined as a non-infective, destructive process affecting bones and joints caused by neuropathy. Risk factors include diabetes, alcoholism, and other conditions causing neuropathy. Clinical presentation varies from swelling in acute cases to structural deformities in chronic cases. Management involves immobilization, bracing, surgery such as fusion or osteotomy to correct deformities, and sometimes amputation for severe cases. Complications can include fractures, deformities, ulcers, and infection.