Downloaded 100 times

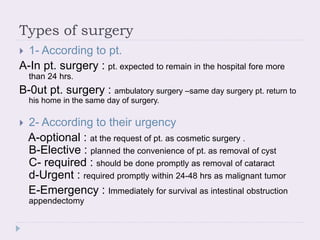
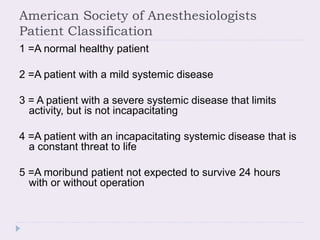
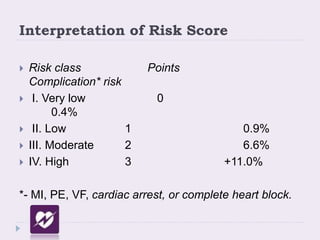

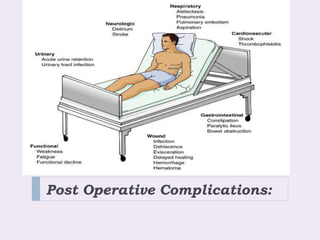


The document discusses peri-operative care, outlining the three phases: pre-operative, intra-operative, and post-operative care. It describes pre-operative care as including patient assessment, history, examinations, investigations, and preparation. Key aspects of pre-operative care are evaluating patient risk factors, medical history, and physical status to determine fitness for surgery and identify risks. The document also discusses classifications of surgery cleanliness and urgency, as well as common post-operative complications.






















































