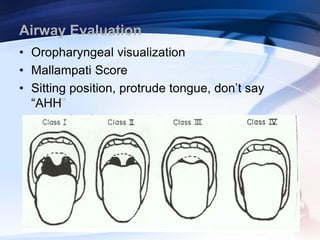
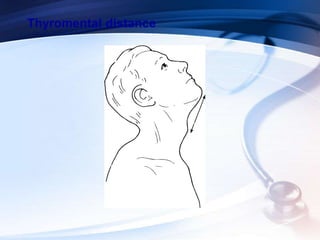
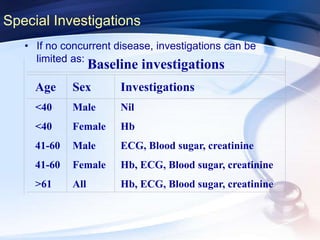
This document discusses the importance of preoperative assessment and premedication in anesthesia. It outlines the goals of the preoperative visit including assessing fitness for anesthesia and optimizing medical conditions. The document describes taking an anesthetic history and physical examination, with a focus on evaluating the cardiovascular, respiratory and airway systems. It discusses using tests like Mallampati scoring and thyromental distance to predict potential airway difficulties. The document also covers determining appropriate preoperative investigations and developing an anesthetic plan tailored to each patient's needs.