Download as PDF, PPTX


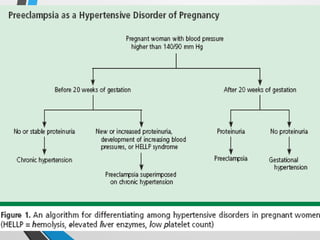
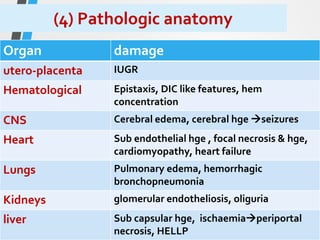
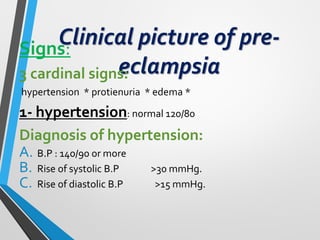
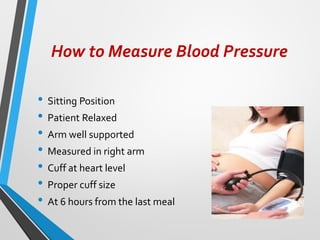

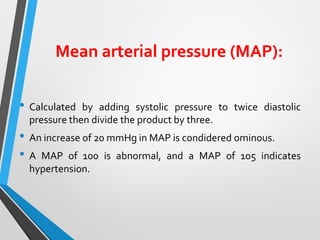
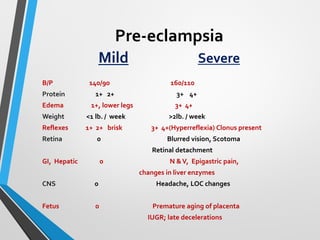
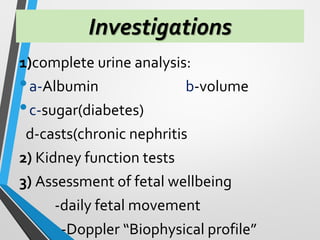
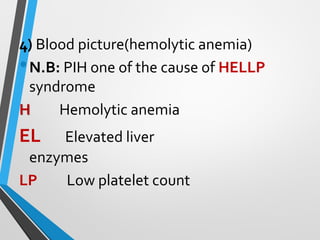
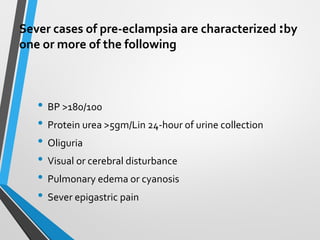




The document outlines pregnancy-induced hypertension, detailing definitions, classifications, causes, and treatments related to hypertensive disorders during pregnancy. It highlights the incidence and consequences of conditions like pre-eclampsia and eclampsia, the diagnostic criteria, and recommended management strategies for both mild and severe cases. Additionally, it addresses the nursing care needed for affected women, emphasizing the importance of monitoring and intervention to improve maternal and fetal outcomes.

















































































