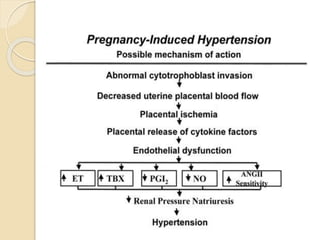
This document discusses pregnancy induced hypertension (PIH), including definitions, classifications, risk factors, pathophysiology, diagnosis, and management. PIH is a multisystem disorder characterized by new onset hypertension after 20 weeks of gestation. It includes gestational hypertension, preeclampsia, and eclampsia. Management involves monitoring for signs of worsening disease and delivering after 37 weeks if mild or earlier if severe to prevent maternal and fetal morbidity and mortality. Treatment includes antihypertensives, magnesium sulfate to prevent seizures, and delivery.







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















