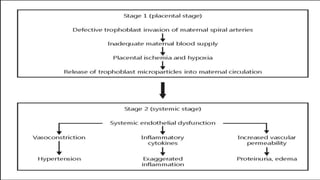
This document discusses pregnancy induced hypertension (PIH), which includes gestational hypertension, pre-eclampsia, and eclampsia. PIH is defined as a rise in blood pressure levels after 20 weeks of gestation. It can be caused by factors like primigravidity, age extremes, diabetes, and others. Pre-eclampsia involves hypertension and proteinuria after 20 weeks. Eclampsia occurs when seizures develop in a woman with pre-eclampsia. Management involves monitoring vitals, delivering the baby if full term, and using magnesium sulfate to prevent seizures. Complications for the mother can include injuries during seizures, pulmonary and renal issues.