This document provides an overview of preclinical drug discovery and development processes. It discusses rational drug design, screening approaches, molecular modification of lead compounds, pharmacokinetic and toxicology studies in animal models, and regulatory requirements for data on a drug's primary pharmacology, secondary effects, and interactions prior to clinical trials. The goal of preclinical research is to obtain sufficient safety and efficacy data on new chemical entities to justify testing in humans.
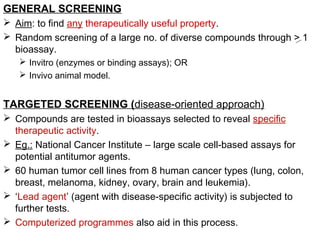
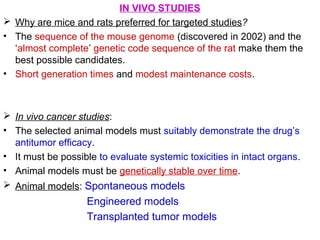
![PHARMACOLOGICAL DATA
Regulatory agencies require the p'cological props. of the
compounds presented in 3 sections:
Primary p’cology
Secondary p’cology
Drug interactions
Primary Pharmacology
Info. on all pharmacological actions relevant to the proposed
therapeutic use.
Guidelines:
• Establish the mechanism of the principal p’cological action (where
possible).
• Validity of animal models should be established. [Models must be
accepted (through literature / earlier similar studies)].
• Results must be in quantitative terms (dose and time-related; to
be correlated with p’cokinetic and p’codynamic data).](https://image.slidesharecdn.com/preclinicaldrugdiscoveryanddevelopment-150928035847-lva1-app6891/85/Preclinical-drug-discovery-and-development-8-320.jpg)






































![Preclinical_Phase_of_Drug_Development_Lucas[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/preclinicalphaseofdrugdevelopmentlucas1-251107071109-7c5cab19-thumbnail.jpg?width=640&height=640&fit=bounds)






















![PHARMACOTHERAPY POINTERS FOR ISCHEMIC STROKE [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ANXIETY & AFFECTIVE DISORDERS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforanxietyaffectivedisordersmalaysiancpgs-230519033737-7916c3bc-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR SCHIZOPHRENIA [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforschizophreniamalaysiancpgs-230519020539-71314b89-thumbnail.jpg?width=640&height=640&fit=bounds)
![PHARMACOTHERAPY POINTERS FOR ATHEROSCLEROSIS [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforatherosclerosismalaysiancpgs-230519014441-00a85dfd-thumbnail.jpg?width=640&height=640&fit=bounds)

![Interpretation of Clinical Lab Data [PFTs] for Newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatapftsfornewbies-230518072330-48aef17c-thumbnail.jpg?width=640&height=640&fit=bounds)
![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)

![TDM POINTERS [GERIATIC & PAEDIATRIC PATIENTS].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/tdmpointersgeriaticpaediatricpatients-230518044517-7b716179-thumbnail.jpg?width=640&height=640&fit=bounds)