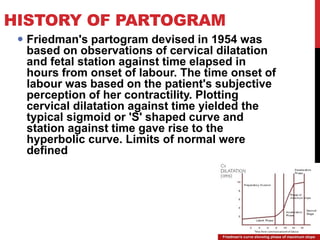
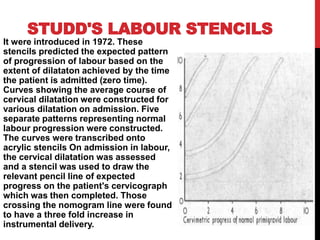
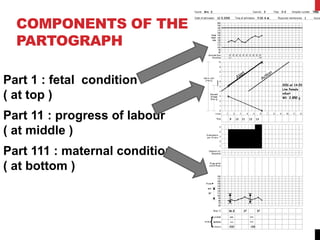
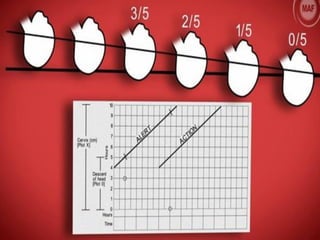
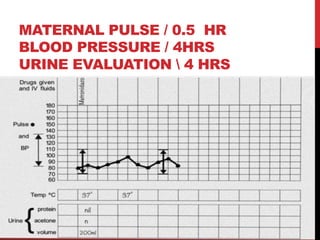
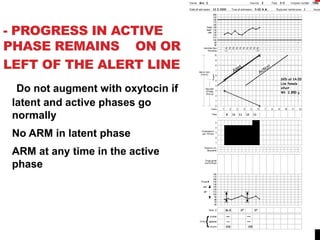
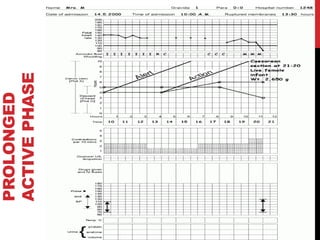
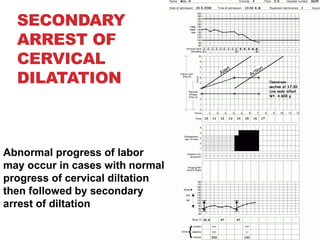
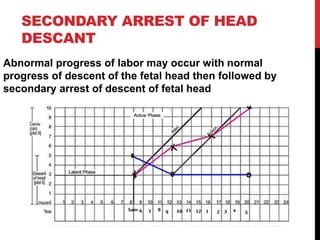
The document discusses the partograph, a tool used to monitor labor progression, originally developed in 1954 by Friedman, and later enhanced by Philpott and Castle. It highlights its components, including fetal and maternal condition monitoring, progress of labor, and the significance of the alert and action lines in managing labor effectively to prevent complications. The partograph plays a crucial role in detecting abnormal labor progression, guiding timely interventions, and improving outcomes for both mother and newborn.