Downloaded 163 times




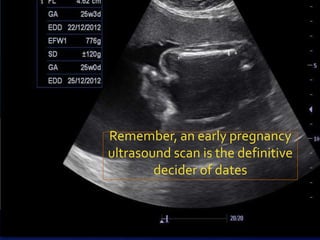


The document discusses discrepancies in uterine size relative to gestational age, highlighting the importance of identifying underlying issues which may relate to the mother, fetus, or placenta. It emphasizes the necessity of confirming pregnancy dates, as well as the need to investigate potential causes such as intrauterine growth restriction, fetal anomalies, or gestational diabetes. Ultimately, a thorough evaluation is crucial before diagnosing a fetus as constitutionally small.























![Grand multiparity hi[12915]](https://cdn.slidesharecdn.com/ss_thumbnails/grandmultiparityhi12915-210509123619-thumbnail.jpg?width=640&height=640&fit=bounds)












































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


