Downloaded 142 times



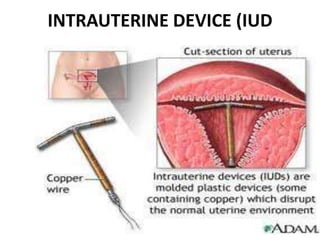
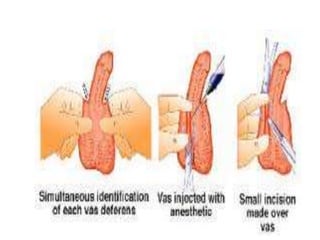

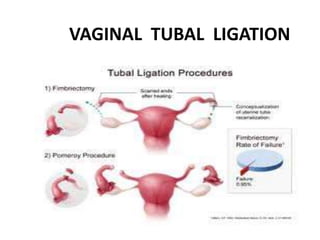


This document provides an overview of emergency and terminal contraceptive methods. It defines emergency contraception as methods that can be used within a few days after unprotected intercourse to prevent pregnancy. Emergency options include emergency contraceptive pills (either a high dose progesterone pill or Yuzpe regimen), copper IUD, or emergency insertion of a contraceptive implant. Terminal methods are intended to be permanent, such as vasectomy for men or tubal ligation for women. Side effects and mechanisms of action are discussed for various emergency and terminal contraceptive options.

































![METHODS_OF_CONTRACEPTION_&_EMERGENCY_CONTRACEPTION[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/methodsofcontraceptionemergencycontraception1-250103093523-49b30cae-thumbnail.jpg?width=640&height=640&fit=bounds)






























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













