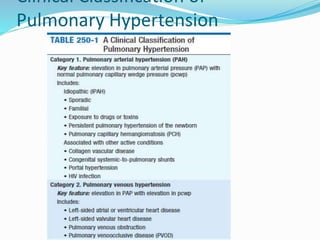
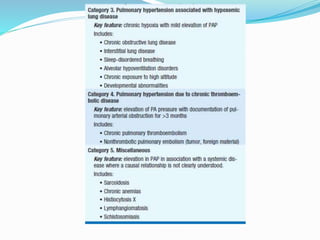
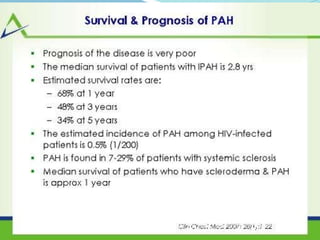
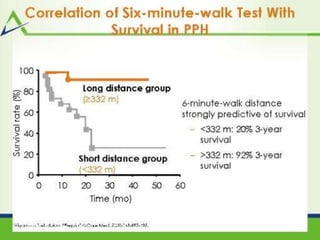
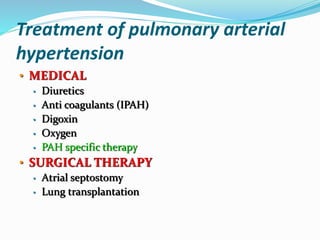
Pulmonary hypertension is defined as a mean pulmonary arterial pressure of at least 25 mm Hg. It can be caused by various conditions and is classified accordingly. Idiopathic pulmonary hypertension has no known cause. It presents with dyspnea and right heart failure. Diagnosis involves right heart catheterization showing elevated pulmonary pressures. Treatment includes diuretics, vasodilators like calcium channel blockers, endothelin receptor antagonists, phosphodiesterase inhibitors, prostanoids, and sometimes atrial septostomy or lung transplantation for severe cases refractory to medical therapy. Prognosis depends on factors like functional status, hemodynamics, and response to treatment.



































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




