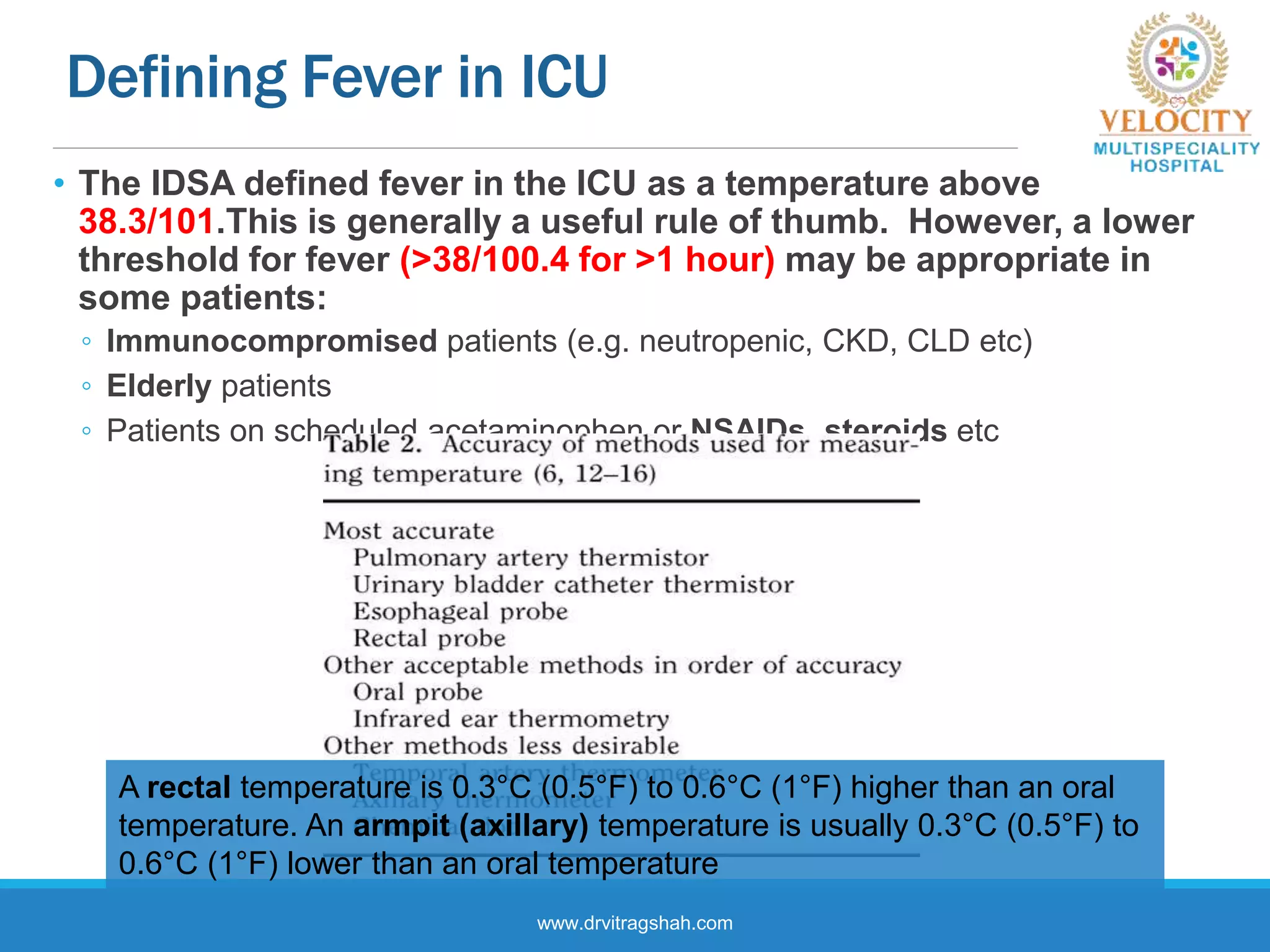
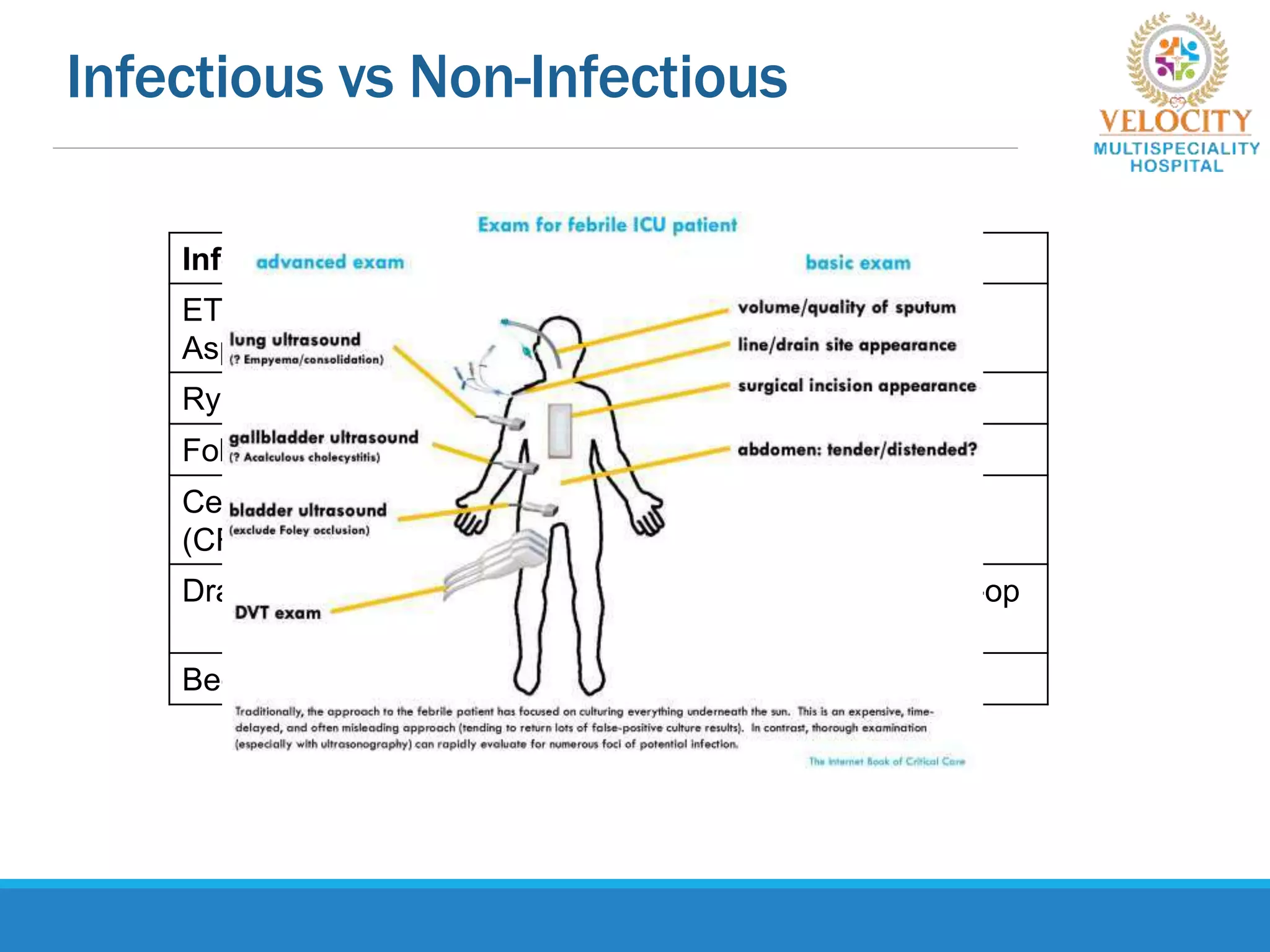
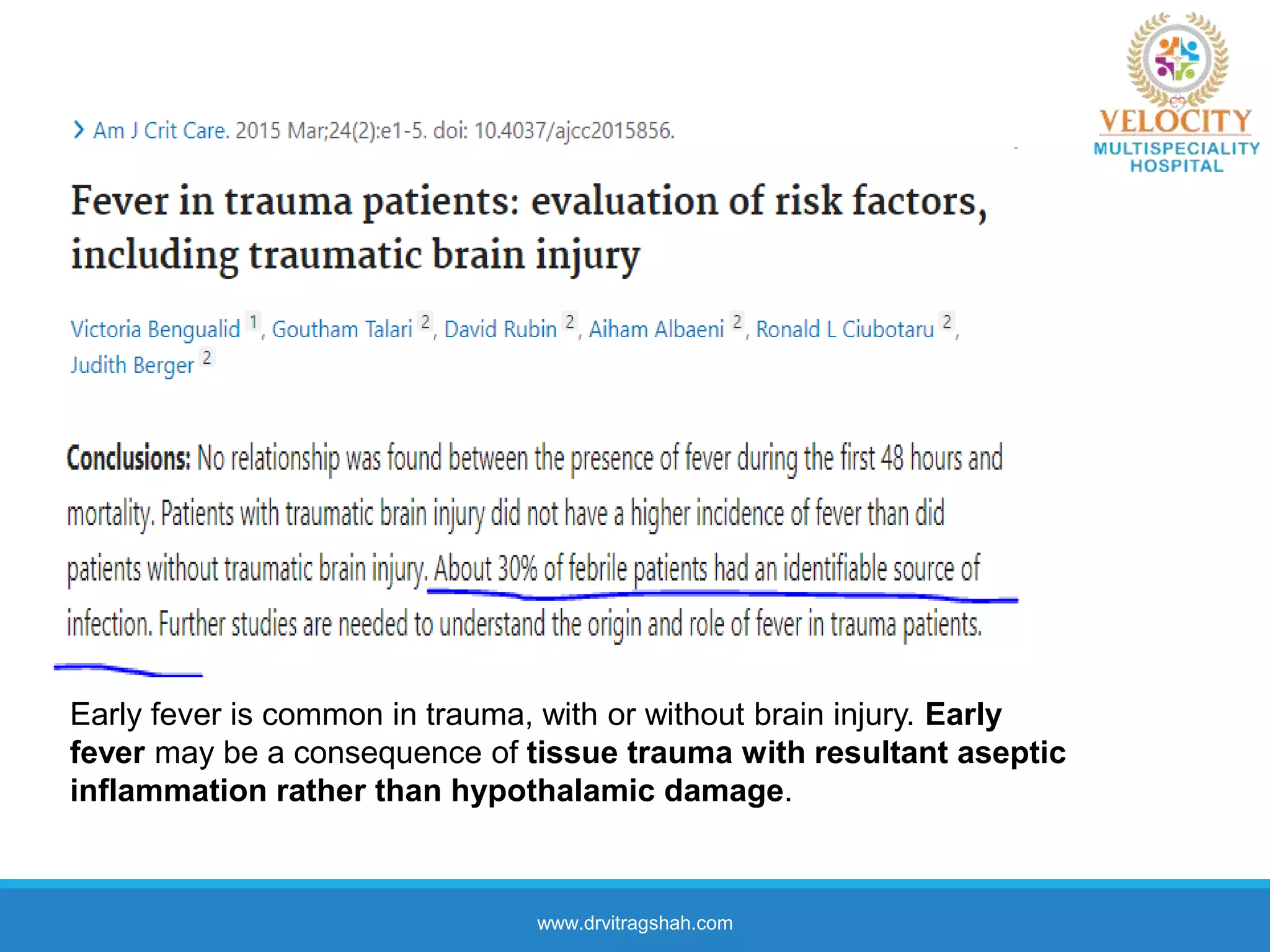
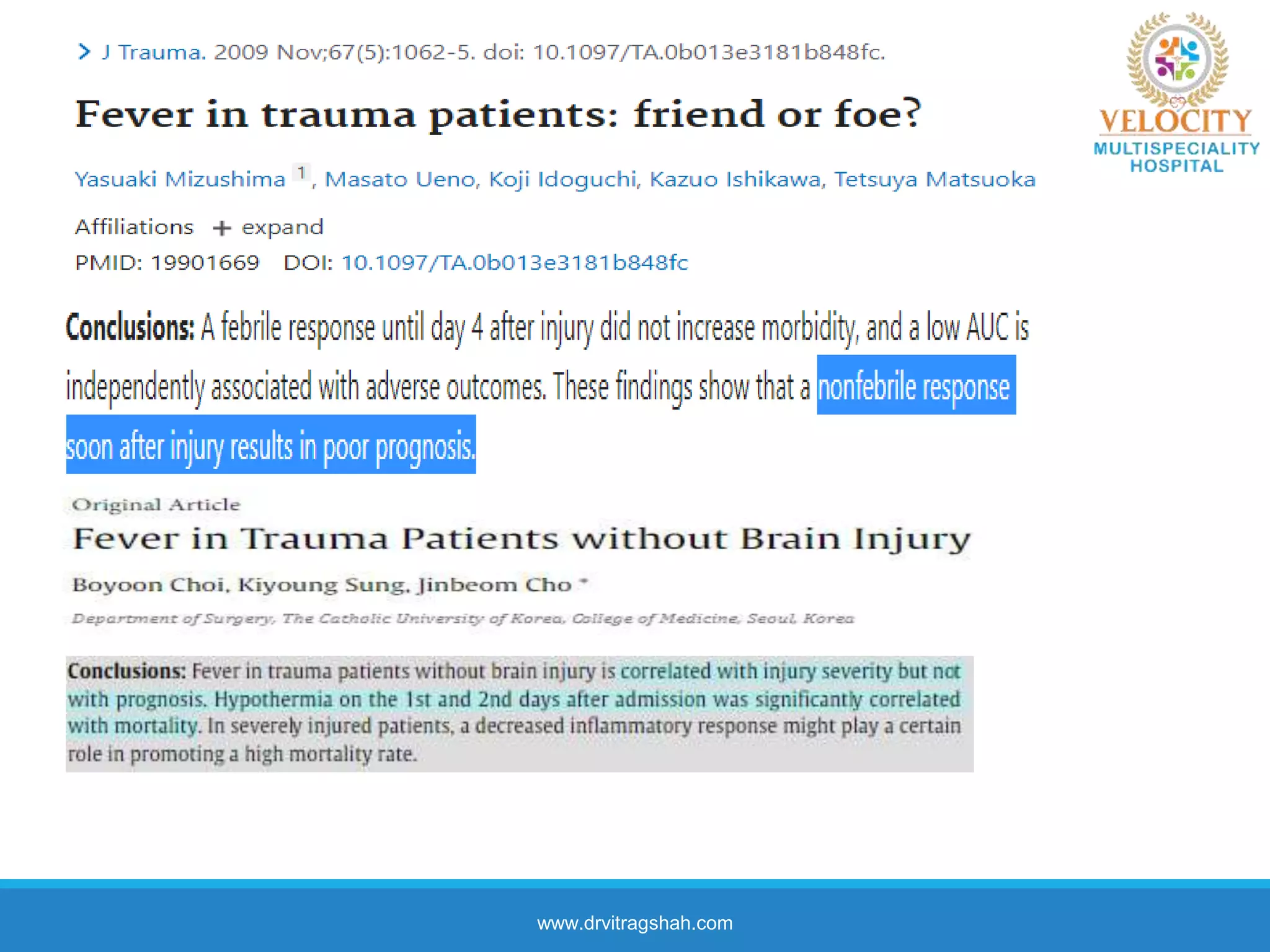
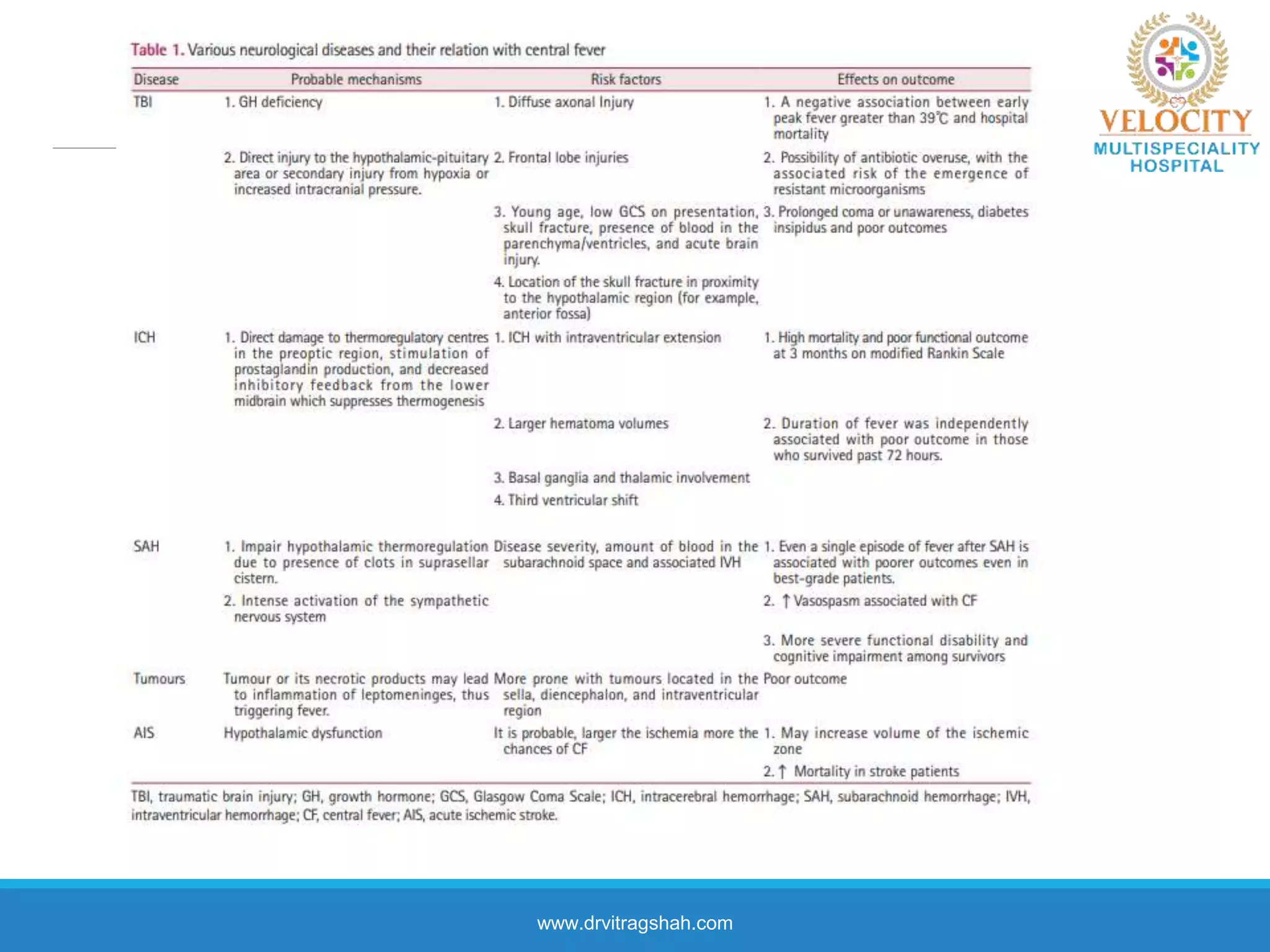
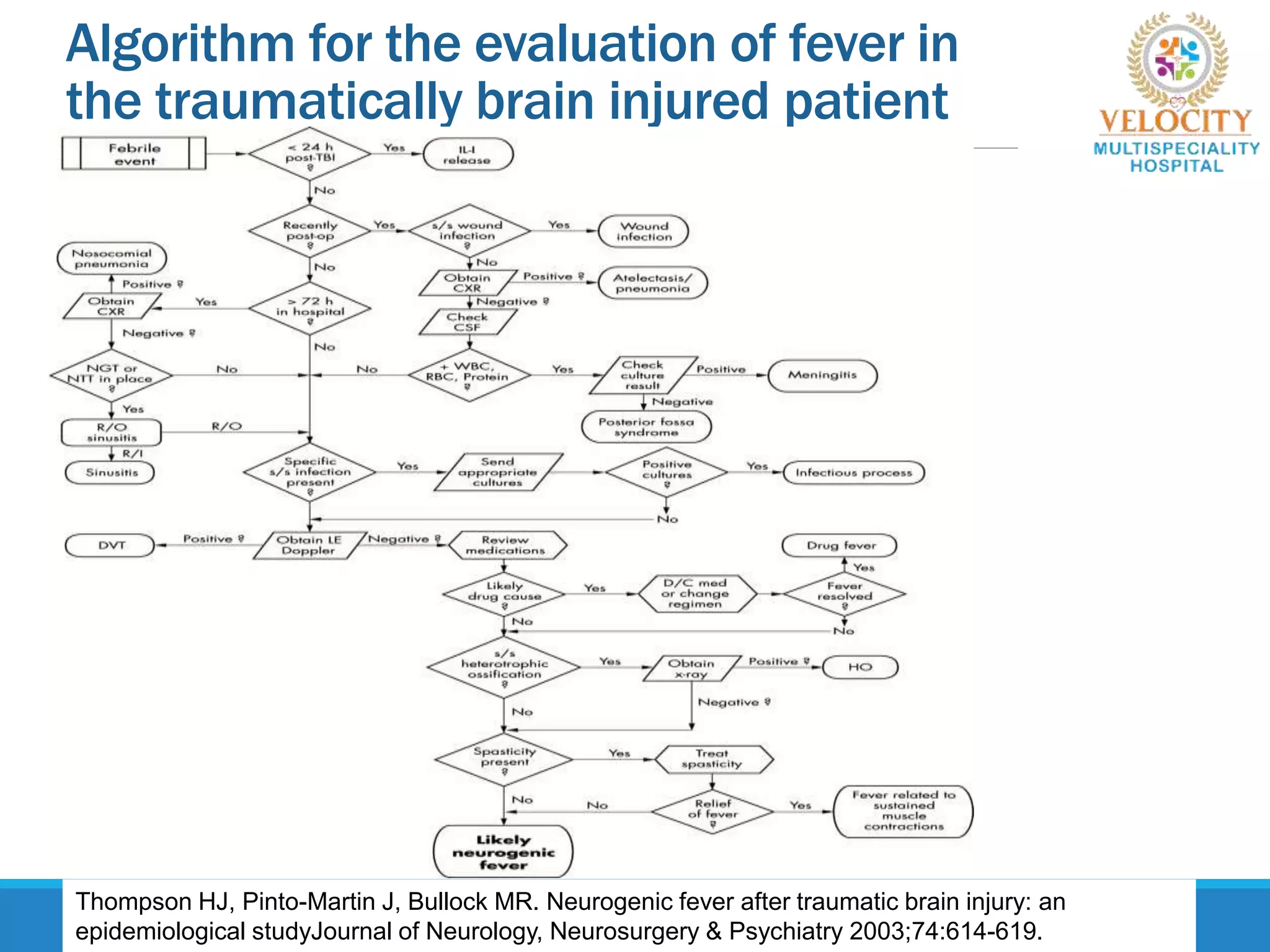
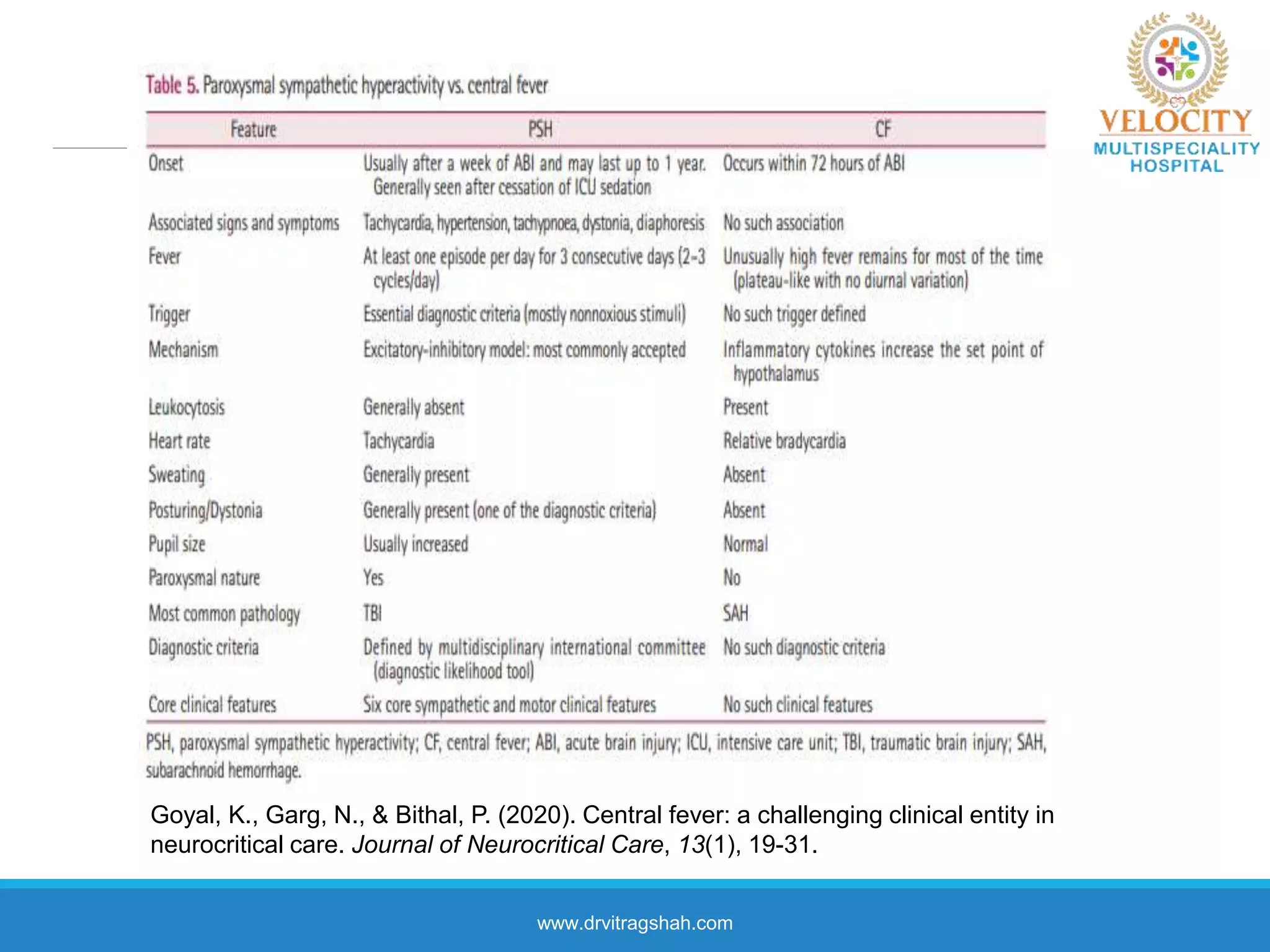
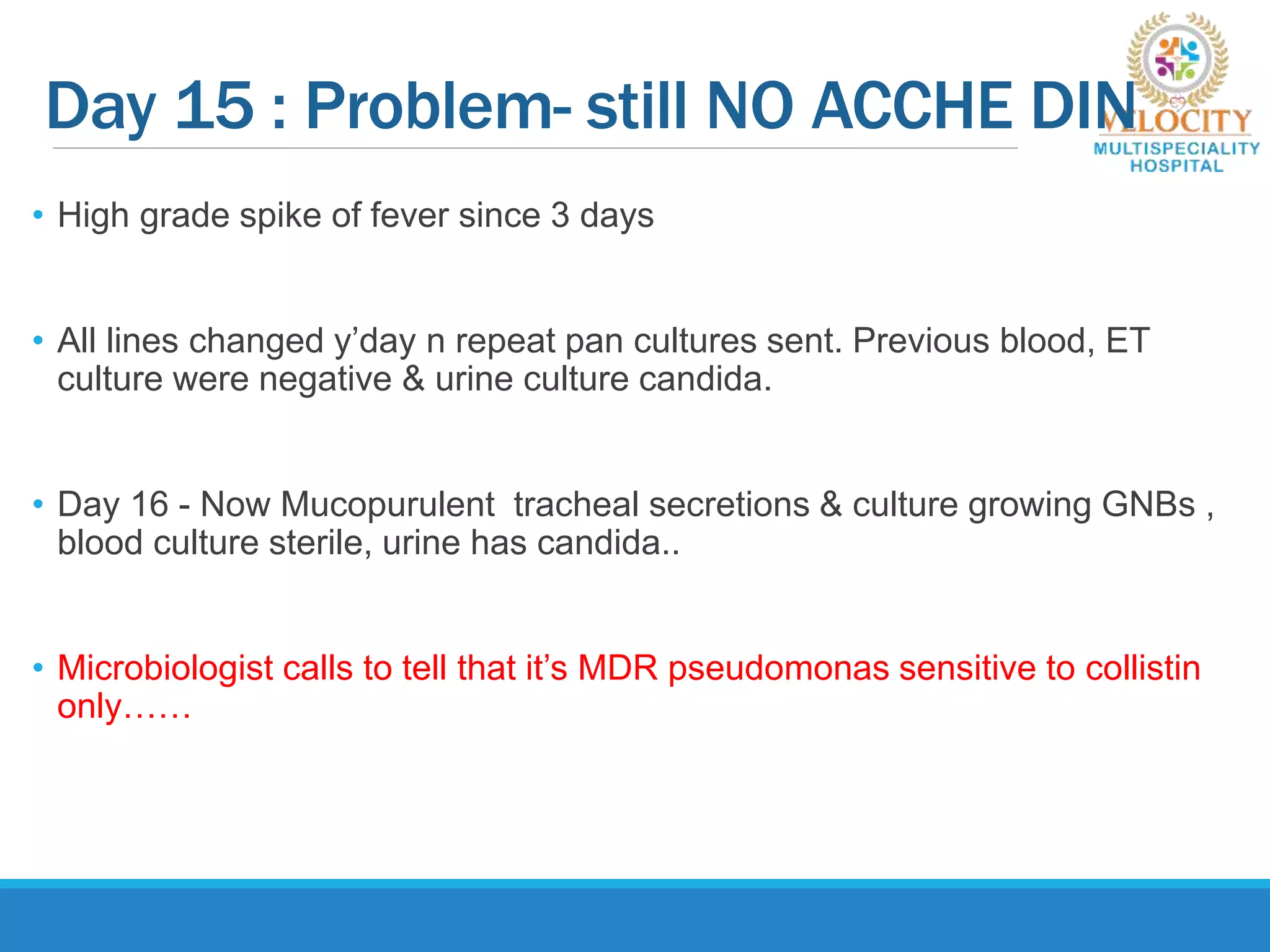
This document discusses the approach to fever in critically ill trauma patients. It defines fever in the ICU and discusses sites for temperature measurement. Both infectious and non-infectious causes of fever are considered. A clinical vignette is presented involving a polytrauma patient with persistent fever. Questions are asked about the potential causes and treatment approach. Central or neurogenic fever resulting from brain injury is described in detail. Postoperative fever and paroxysmal sympathetic storms are also explained. The case progresses over multiple days, discussing treatment challenges and decisions. Reflection on diagnostic versus antibiotic-focused approaches to fever is provided.