Downloaded 208 times

![POST CESAREAN PREGNANCY
• Pregnancy with history of previous caesarean
section
• Caesarean section rate – 8 to 25%
[Increase in the incidence of CS rate is
because of liberal and expanded
indications]](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-2-320.jpg)
![Cesarean Section [CS] - Indications
1) Labour dystocia – Arrest of cervical dilatation or
arrest of foetal descent
2) Breech presentation – Malpresentation
3) Foetal distress – Foetal heart abnormalities,
Hypoxia/ Acidosis and Meconium stained
liquor [MSL]
4) Previous caesarean pregnancy
5) Others – APH [Accidental haemorrhage and
Placenta praevia], Severe PIH and IUGR](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-3-320.jpg)

![6/7/2015 hcb 7
Type and Incidence of Scar Rupture
S.No Type of Scar Incidence of scar
rupture
1 Upper segment –[Classical] 4 – 9 %
2 Lower segment:-
a Low vertical 1 – 7 %
b* Low Transverse [LSCS] 0.2 – 1.5 %
3 T – shape scar 4 – 9 %](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-7-320.jpg)
![6/7/2015 hcb 8
Previous Uterine Scar Behavior
LSCS [Lower segment
Transverse Scar] –
1.Thin margins – better
apposition
2.Suture line undisturbed –
passive segment [stretch
and relax]
Classical [Upper segment
Vertical Scar] –
1.Thick margins - apposition
unsatifactory
2. Loosening of sutures – active
segment [contract and
retract]](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-8-320.jpg)
![6/7/2015 hcb 10
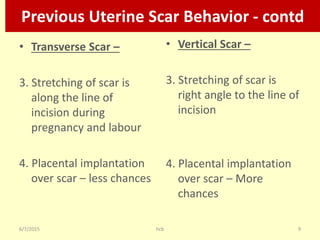
Previous Uterine Scar Behavior - contd
• Transverse Scar –
5. Scar rupture rate:- 0.2 to
1.5% [Sound scar, scar
ruptures during labour and
less incidence of maternal
& foetal mortality]
• Vertical Scar –
5. Scar rupture rate: 4 to 9%
[Weak Scar, scar ruptures
during pregnancy and
labour; more incidence of
maternal & foetal
mortality]](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-10-320.jpg)
![6/7/2015 hcb 14
Vaginal Birth After Cesarean [VBAC]
• Rupture of uterus during pregnancy or labour
can be catastrophic, therefore VBAC should
be attempted in a well equipped institution
only
• Where services of Obstetrician,
Anaesthesiologist, Neonatologist are available
and safe blood can be transfused to the
patient if required](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-14-320.jpg)
![6/7/2015 hcb 18
Uterine Scar Rupture - Signs
1. Maternal tachycardia and hypotension
2. Foetal heart variability [decelerations]
3. Uterine scar tenderness
4. Failure of progress of labour [arrest of descent
of foetal parts]](https://image.slidesharecdn.com/postlscspregnancy-150607123927-lva1-app6892/85/Post-lscs-pregnancy-18-320.jpg)

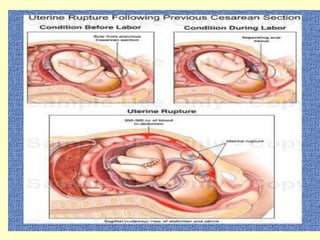
1. The document discusses post-cesarean pregnancy and management options. Women with a previous cesarean section have an increased risk of complications during subsequent pregnancies like scar rupture or dehiscence. 2. Trial of vaginal birth after cesarean (VBAC) can be attempted if the first cesarean section was low transverse and facilities for emergency cesarean are available. Risk factors like classical or inverted-T incisions or medical complications contraindicate VBAC. 3. Close monitoring during labor is needed for VBAC due to risks of uterine rupture which can be life-threatening for the mother and baby if not recognized promptly. Elective repeat cesarean is recommended if VB

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





