Download to read offline
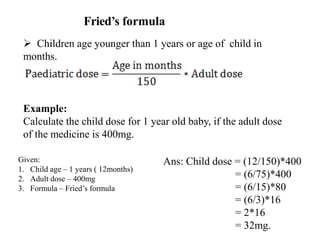
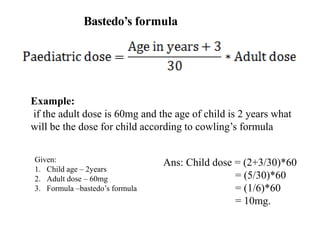
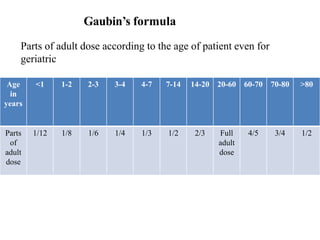
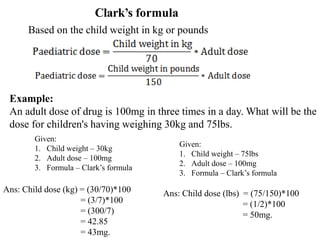


This document discusses posology, which is the science of determining safe and effective drug doses. It explains that the dose is usually expressed as a range, with a minimum dose to produce the intended effect and a maximum tolerated dose. Many factors affect the appropriate dose for a given patient, including age, sex, pregnancy status, body weight, disease severity, route of administration, and genetic differences. Close monitoring of these factors is needed to determine a safe individualized dosage.




































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















