Download as PDF, PPTX








































![• At steady state. The rate of change of amount of drug in the body is zero,eq
23 becomes
Zero=ro-kexss
Kexss=ro
Css=ro/kevd
=Ro/clt i.E
…27
…28
…29
infusion rate ....30
…31
Clearance
Substituting eq. 30 in eq. 26
•C=css(1-e-ket)
Rearrangement yields:
• [Css-c]=e-ket
. ...32
…33
Css
Log CSS-C
Css
= -ket
2.303](https://image.slidesharecdn.com/pharmacokinetics-250121143141-1cfe9098/75/BIOPHARMACEUTICS-AND-PHARMACOKINETICS-pdf-43-2048.jpg)
![• If n is the no. Of half lives passed since the start of infusion(t/t1/2)
• Eq. Can be written as
• C=CSS [1-(1/2)n] …34](https://image.slidesharecdn.com/pharmacokinetics-250121143141-1cfe9098/75/BIOPHARMACEUTICS-AND-PHARMACOKINETICS-pdf-44-2048.jpg)



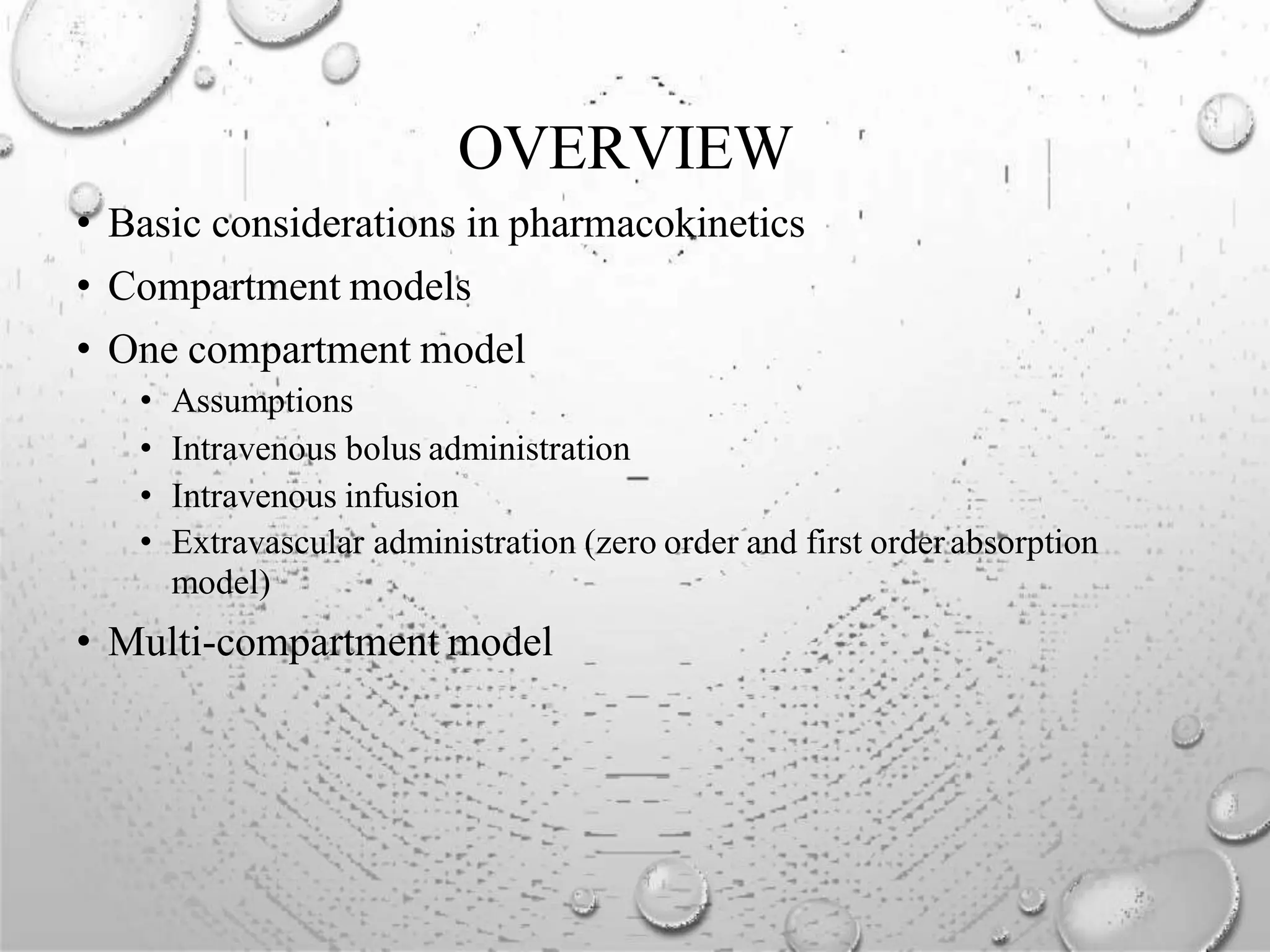
![ONE COMPARTMENT MODEL: EXTRA
VASCULAR ADMIN ( FIRST ORDER
ABSORPTION)
Blood & other
Body tissues
Drug at
site
KE
Ka
First order
absorption
elimination
• Drug that enters the body by first order absorption process gets distributedin
the body according to one compartment kinetic and is eliminated by first
order process.
• The model can be depicted as follows and final equation is as follows
C=Ka F Xo/Vd(Ka-KE) [e -Ket-e-Kat] …41](https://image.slidesharecdn.com/pharmacokinetics-250121143141-1cfe9098/75/BIOPHARMACEUTICS-AND-PHARMACOKINETICS-pdf-48-2048.jpg)

The document is an educational outline focused on biopharmaceutics and pharmacokinetics, specifically detailing pharmacokinetic models and parameters crucial for understanding drug kinetics in the body. It covers topics such as pharmacokinetic and pharmacodynamic parameters, various modeling approaches, and the mathematical representation of drug behavior post-administration. Key pharmacokinetic concepts like volume of distribution, clearance, and the significance of half-life are emphasized, along with practical applications in drug dosing and bioavailability assessment.























































































