Downloaded 24 times
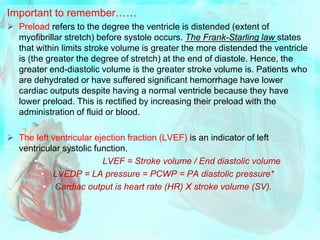
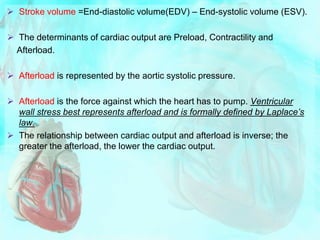
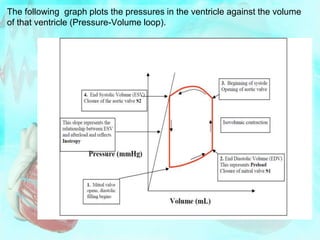
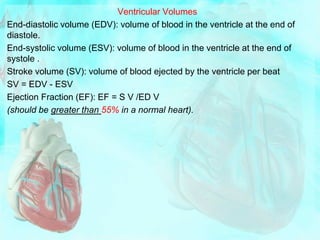

This document summarizes cardiac muscle mechanics and the cardiac cycle. It describes how cardiac muscle operates on the ascending limb of the active tension curve, allowing force of contraction to increase with stretching. It then outlines the key components and phases of the cardiac cycle from both mechanical and electrical perspectives. This includes definitions of systole, diastole, and the isovolumic phases. Pressure and volume relationships throughout the cycle are depicted in diagrams. Factors influencing cardiac performance like preload, contractility, and afterload are also defined.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











