Downloaded 54 times

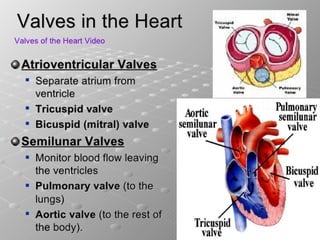


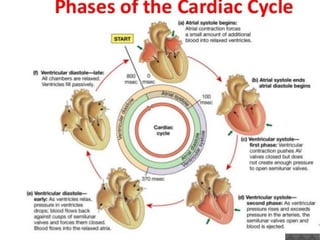












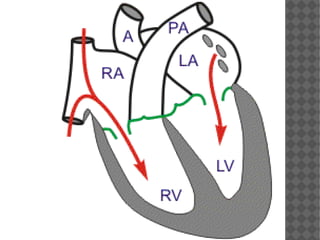


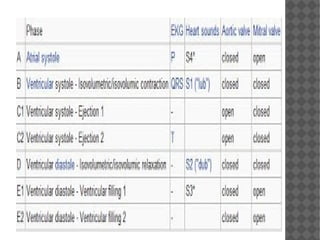


The cardiac cycle consists of two main phases - diastole and systole. During diastole, the ventricles relax and fill with blood from the atria through the open atrioventricular valves. Atrial contraction occurs at the end of diastole, pushing additional blood into the ventricles. Systole begins with ventricular contraction, causing the atrioventricular valves to close and isolating the ventricles as pressure rises. When pressure exceeds that in the arteries, the semilunar valves open and ejection occurs, followed by their closing as pressure falls at the end of systole. The cycle then repeats with rapid ventricular filling and relaxation.




















































































