The document discusses the anatomy of the shoulder joint, including the bones, ligaments, and motions. It describes:
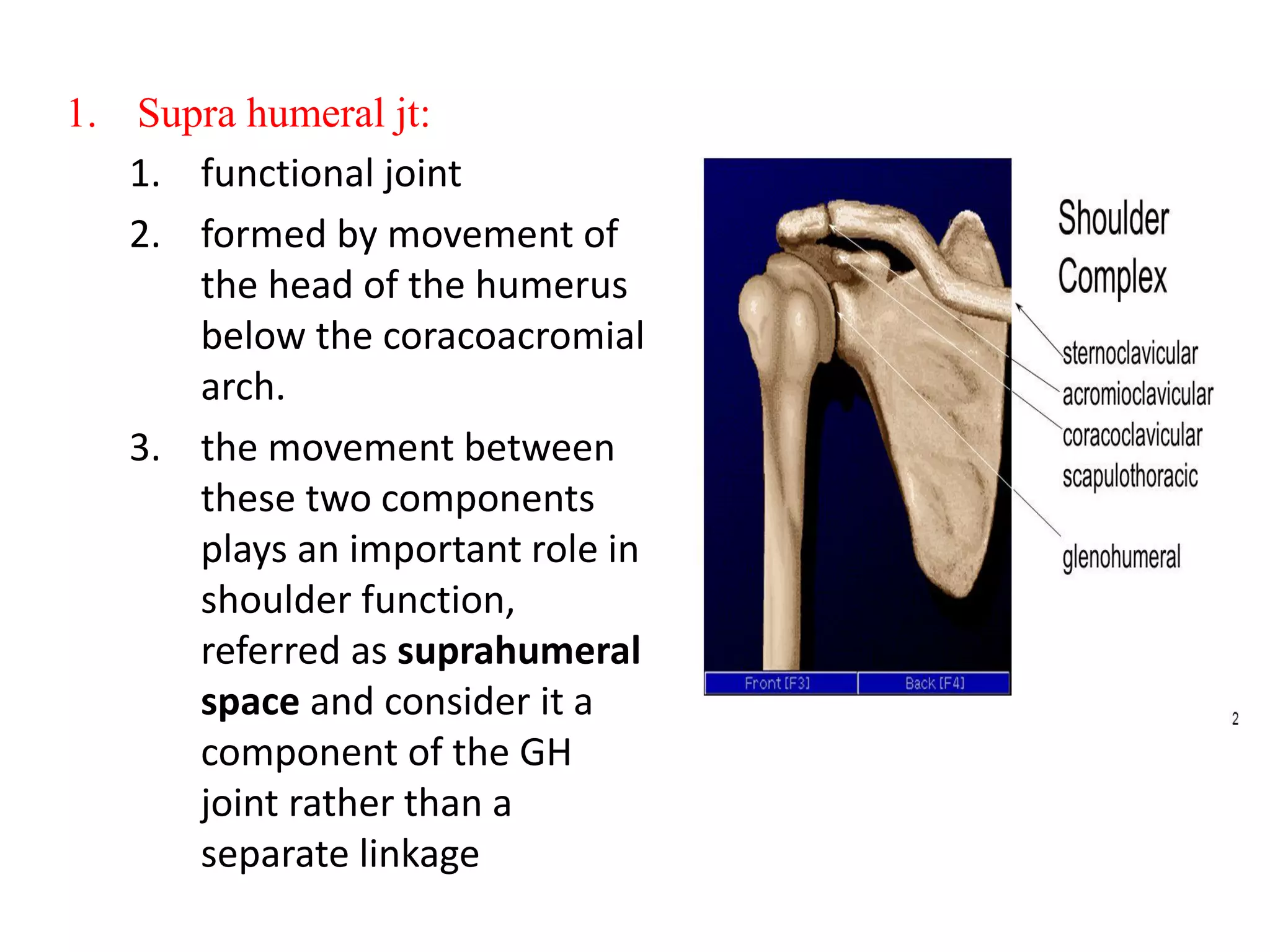
1. The shoulder joint is a ball-and-socket joint formed by the humeral head and glenoid fossa. It allows multidirectional movement but has less stability than other joints.
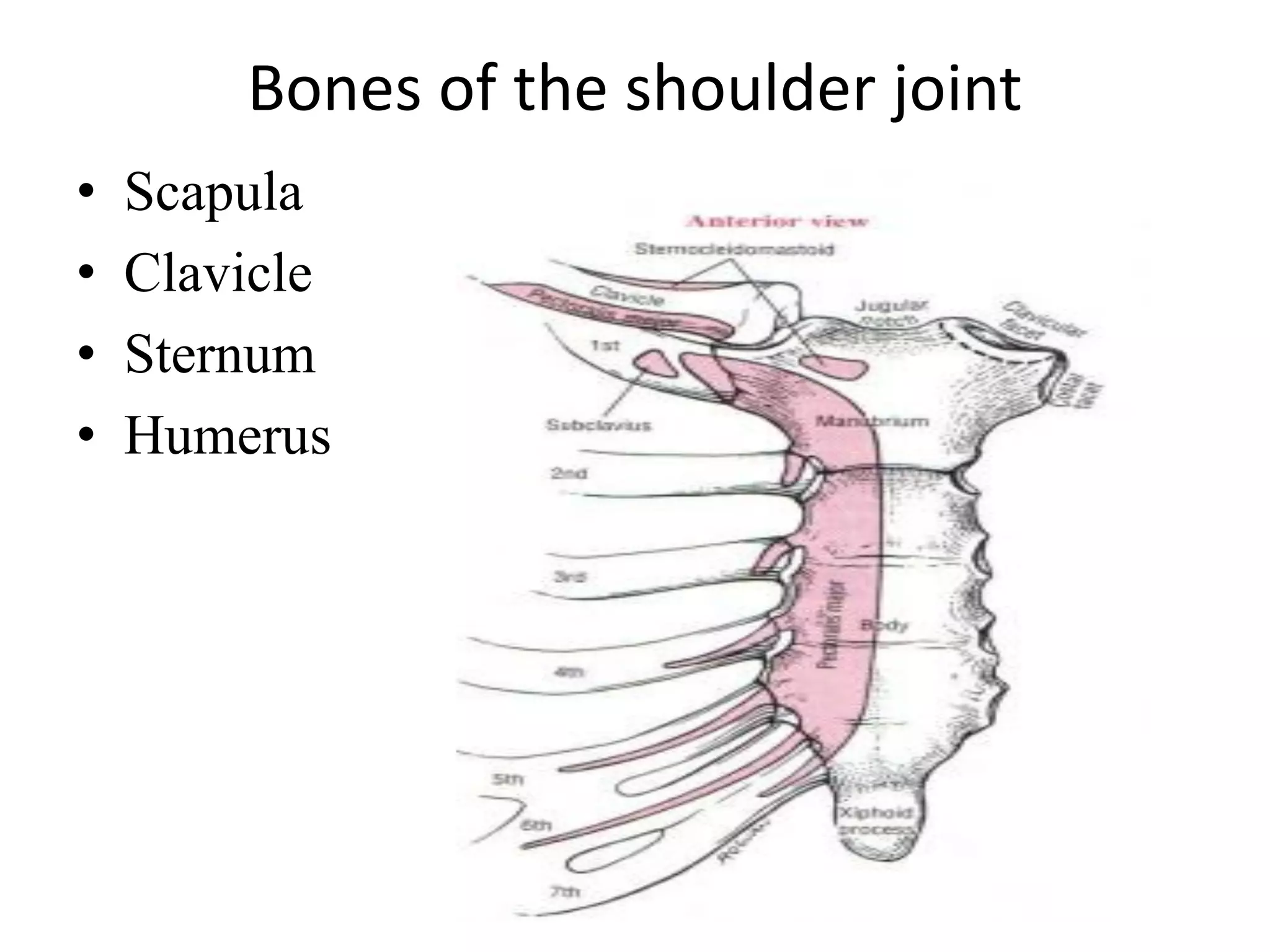
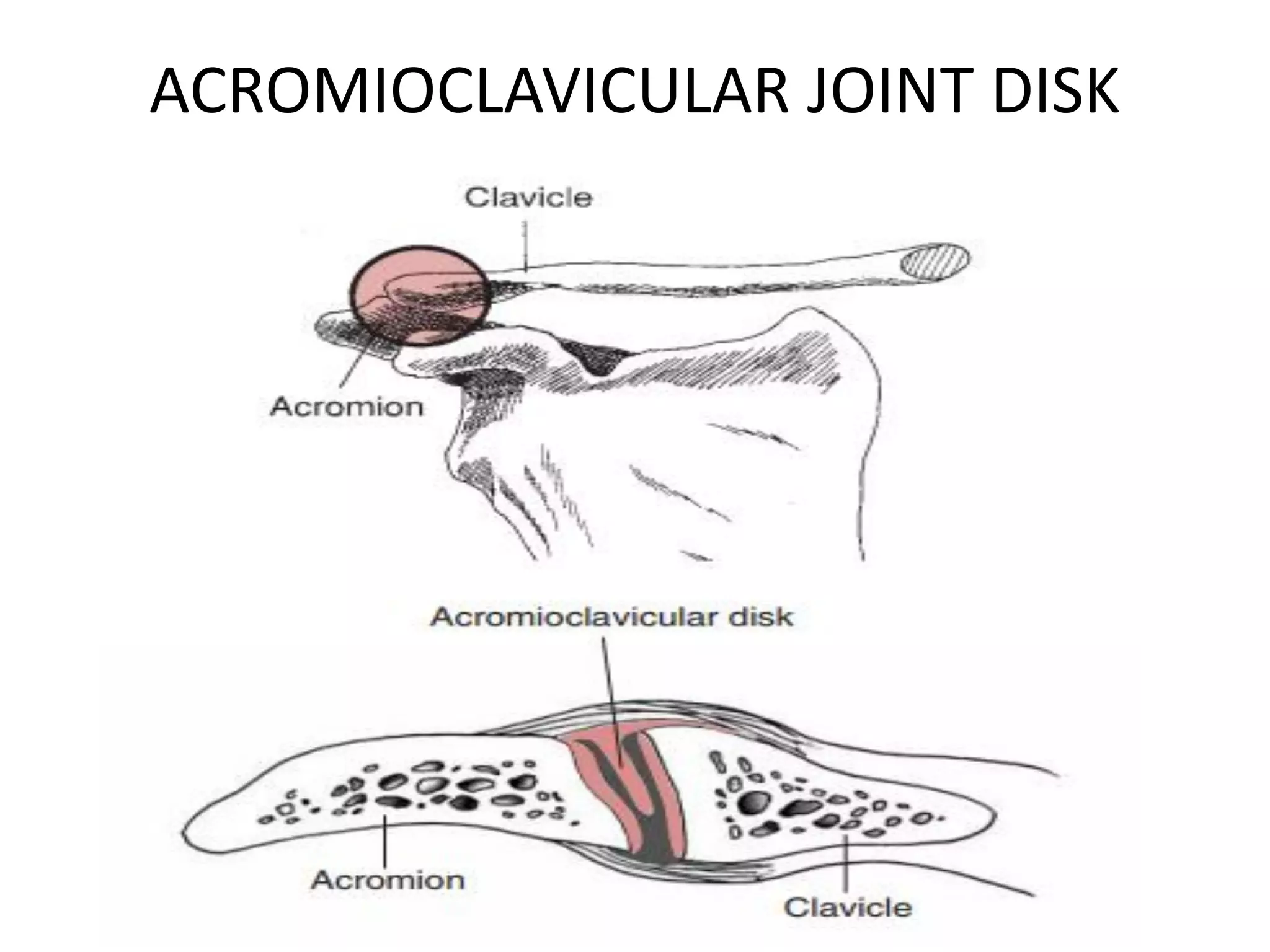
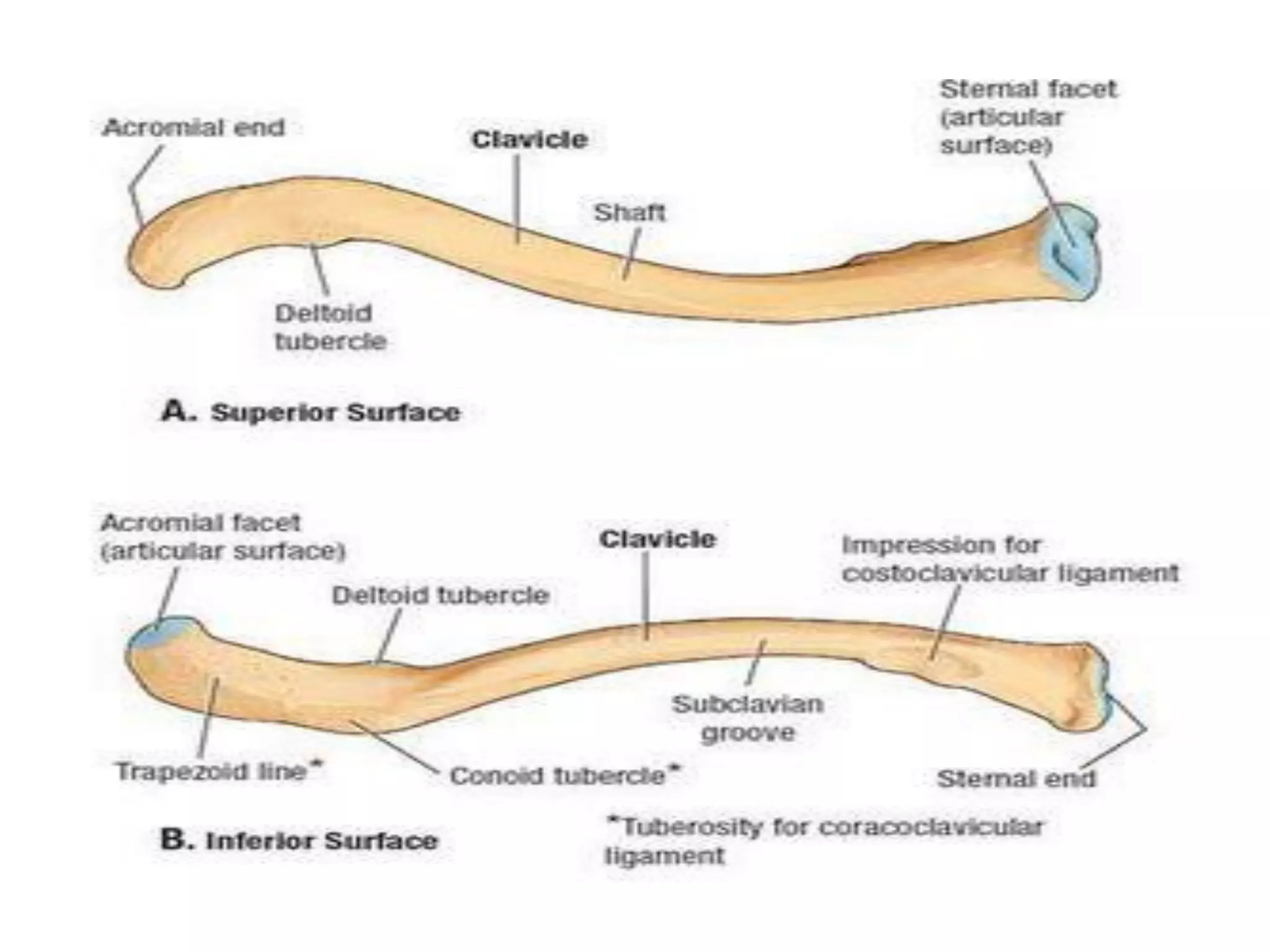
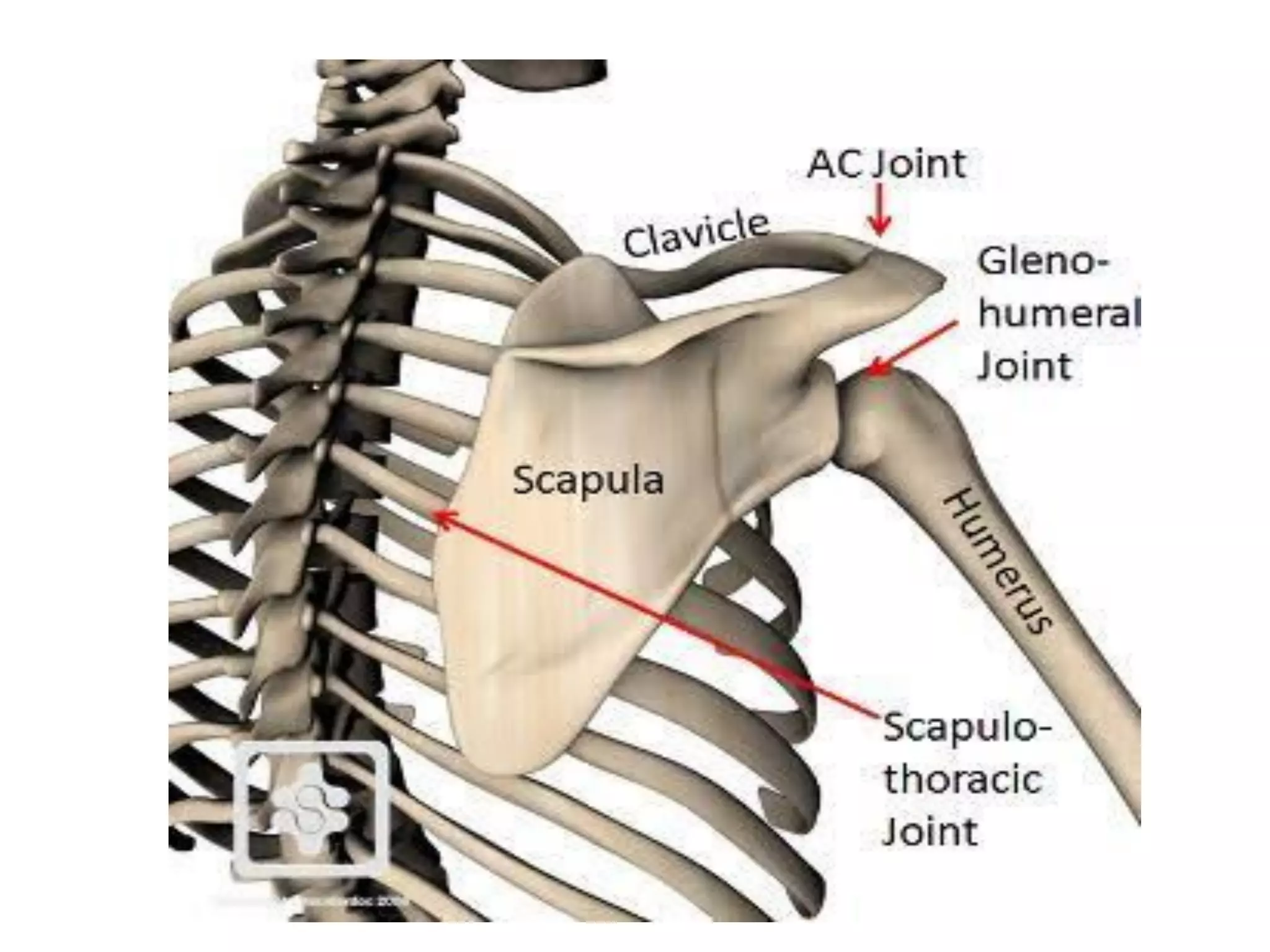
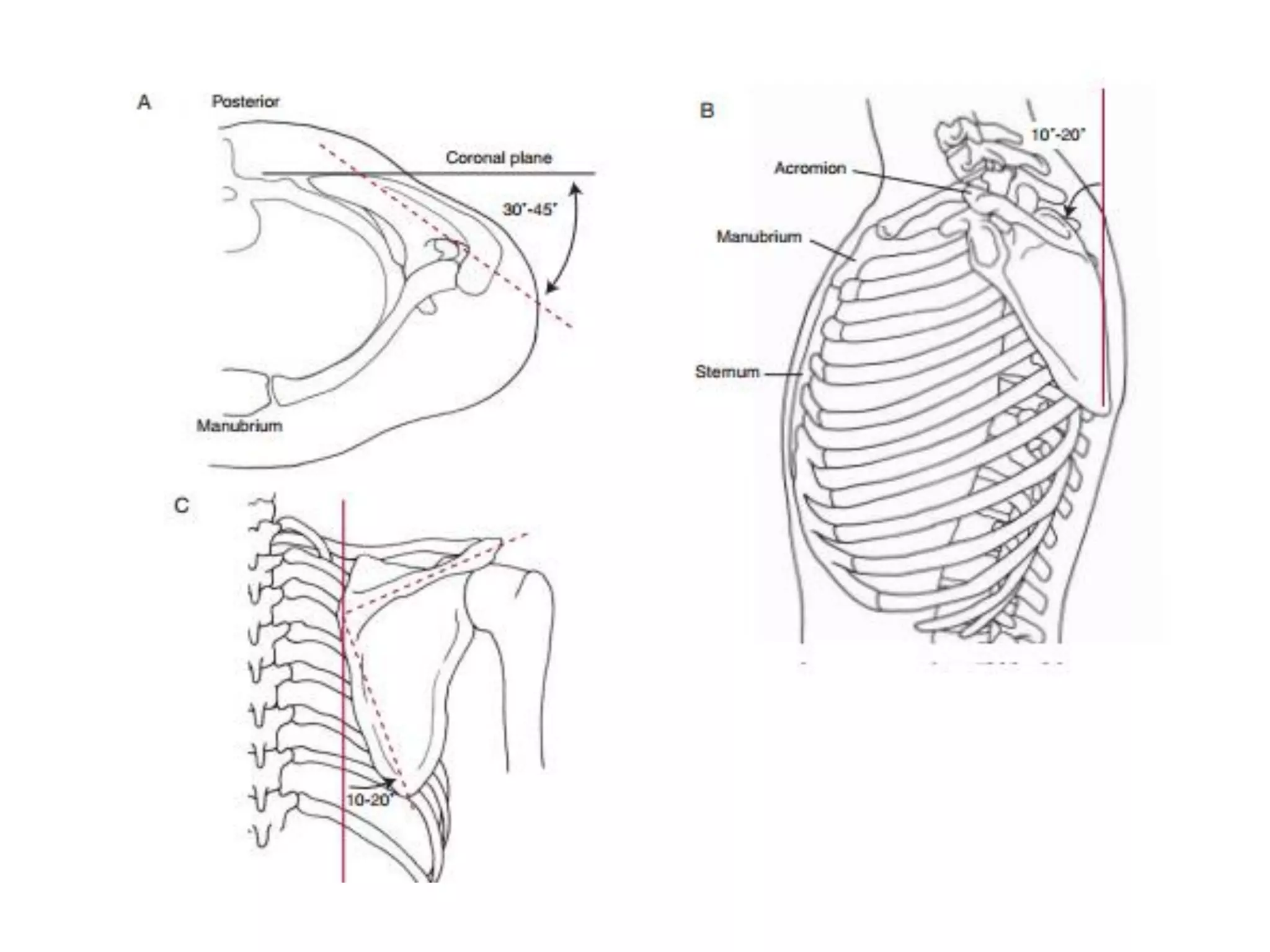
2. Key bones include the scapula, clavicle, and humerus. The glenoid fossa is shallow and reinforced by the glenoid labrum. The humeral head is retroverted to increase congruence with the glenoid.
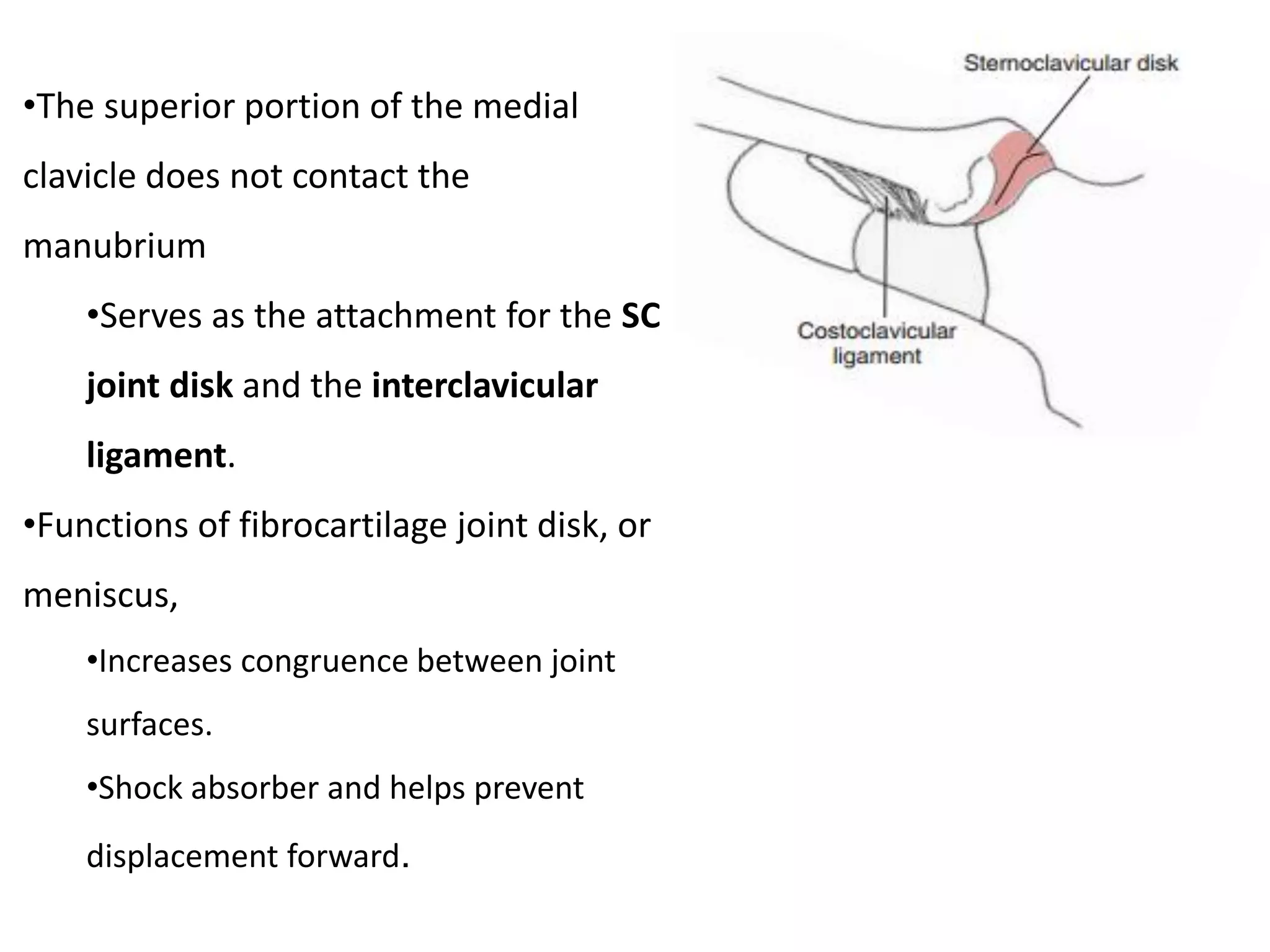
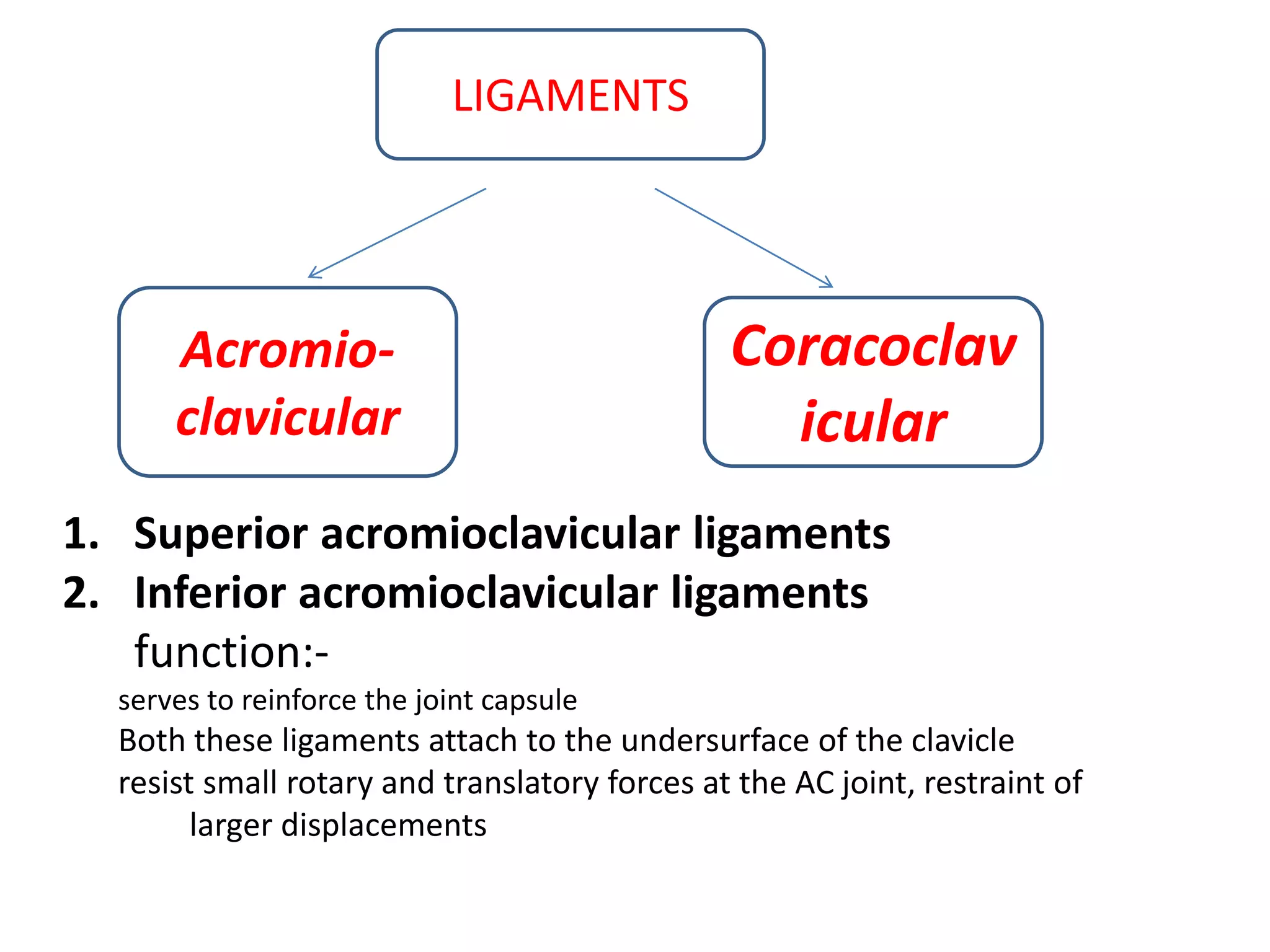
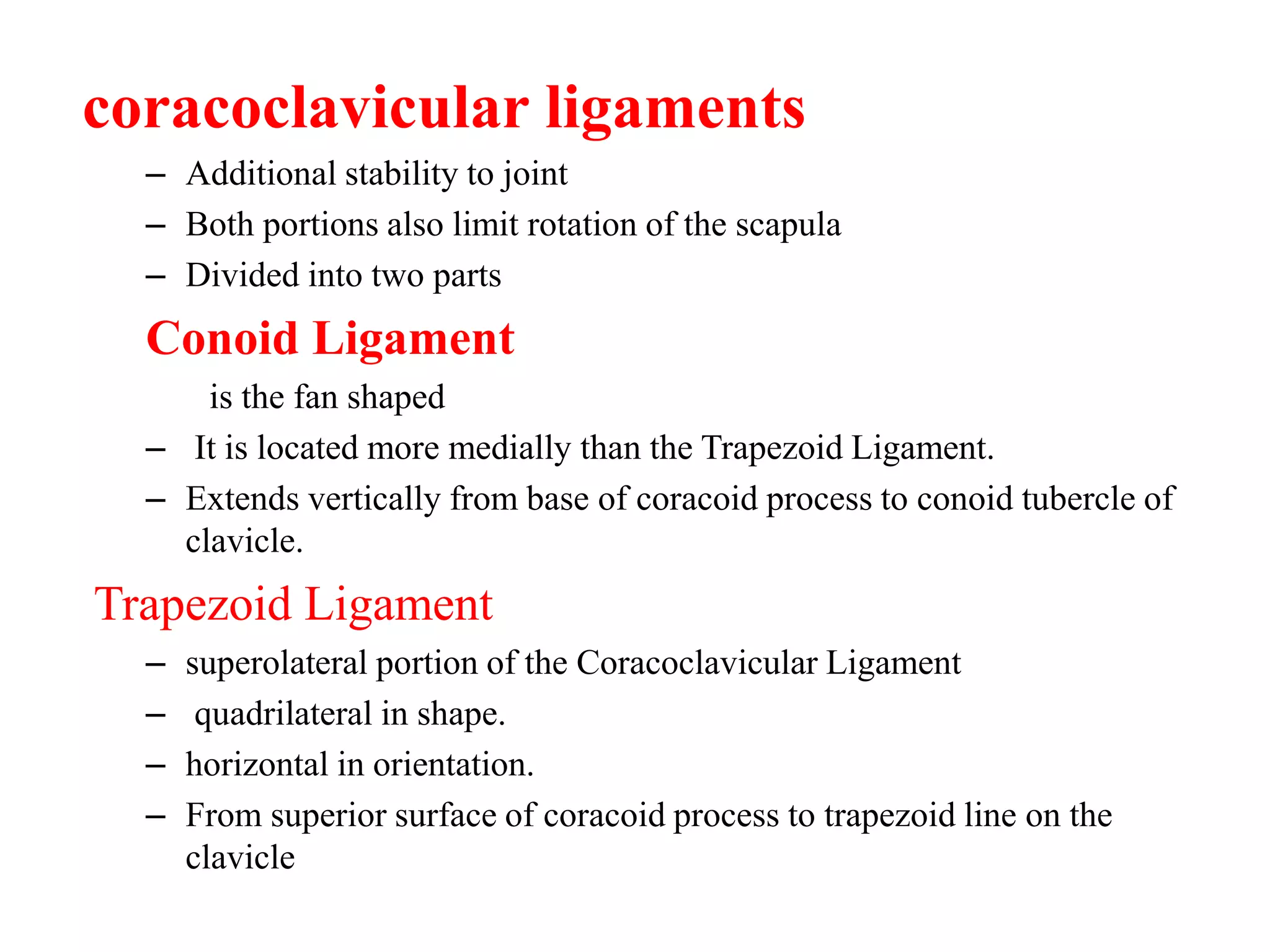
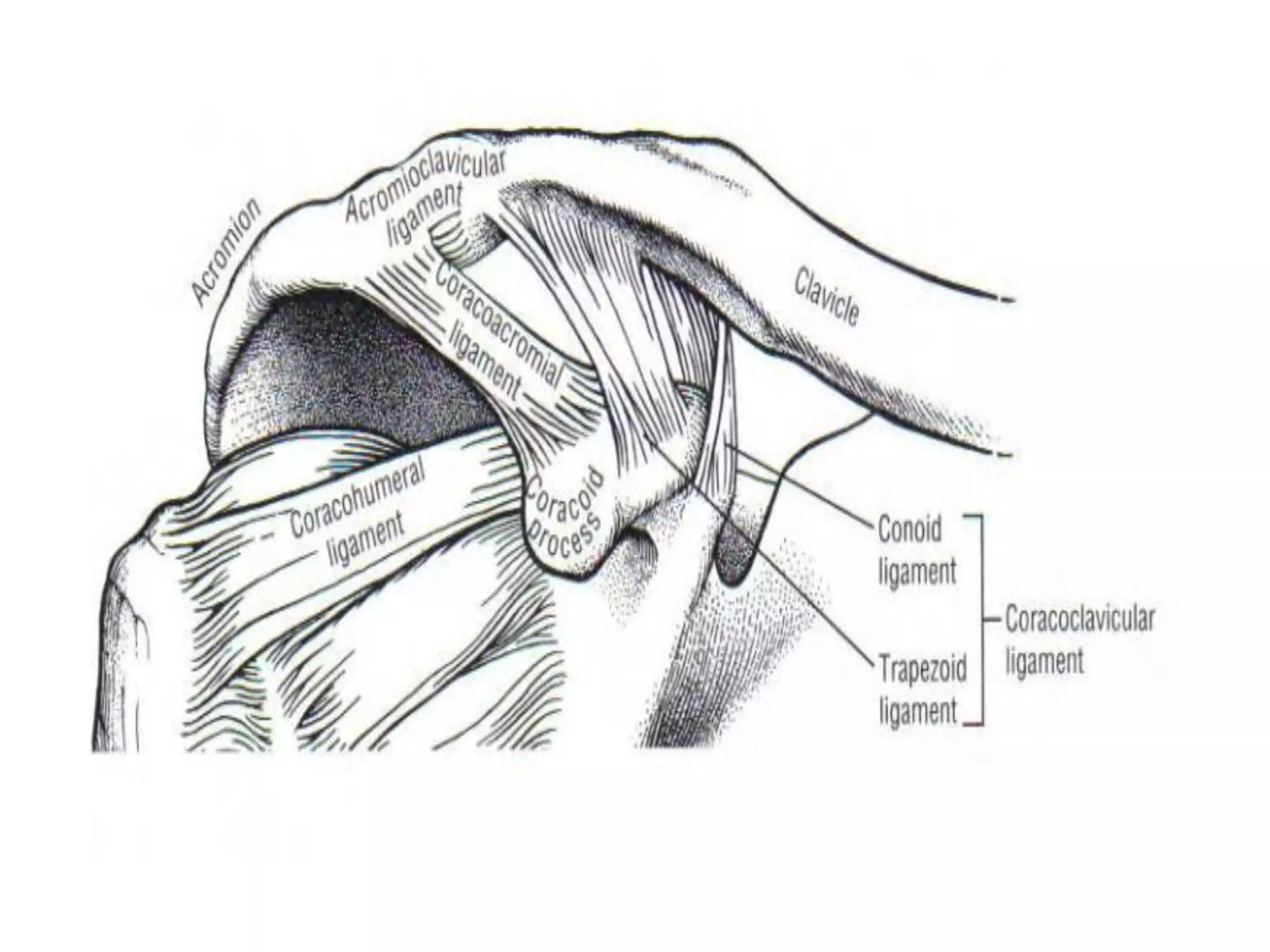
3. Ligaments like the glenohumeral, coracohumeral and rotator cuff