Downloaded 939 times

















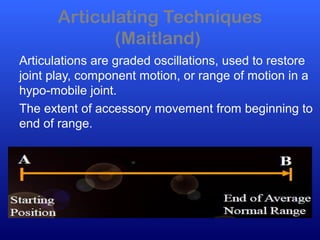
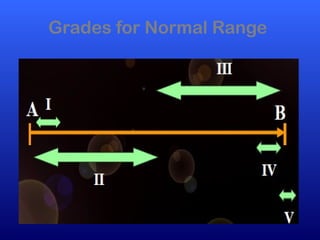
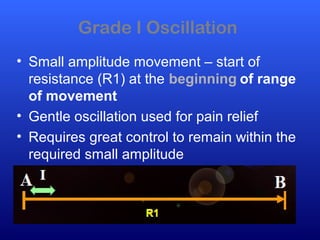
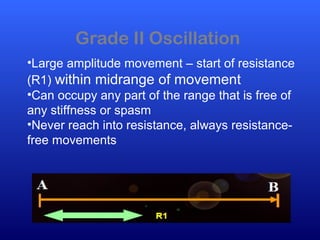
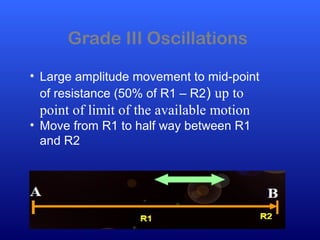

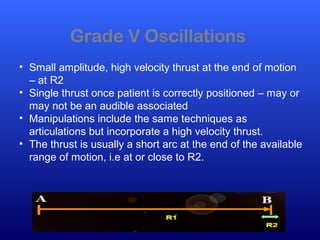
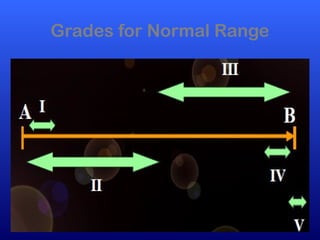
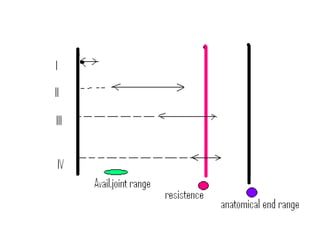





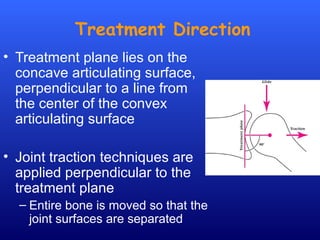
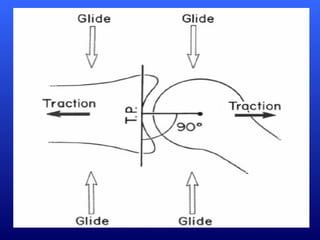




This document defines joint mobilization techniques and provides guidelines for their use. It describes mobilization as a manual therapy that uses passive joint movement to increase range of motion or decrease pain. Accessory joint movements like gliding and traction are explained. Precautions and contraindications for mobilization are outlined. A grading scale from I to V is presented to indicate the amplitude of oscillations used in different mobilization techniques.