Downloaded 42 times











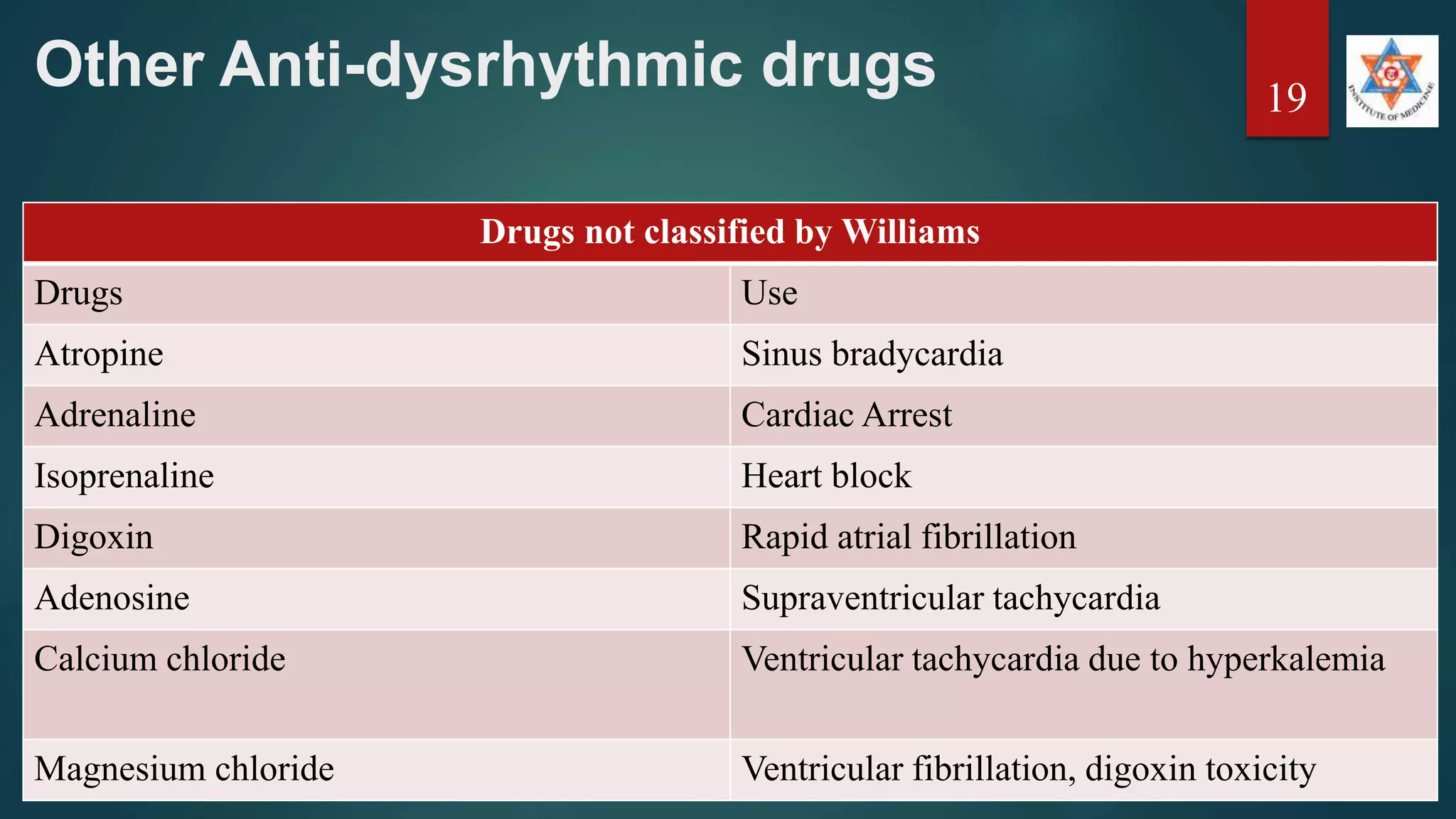
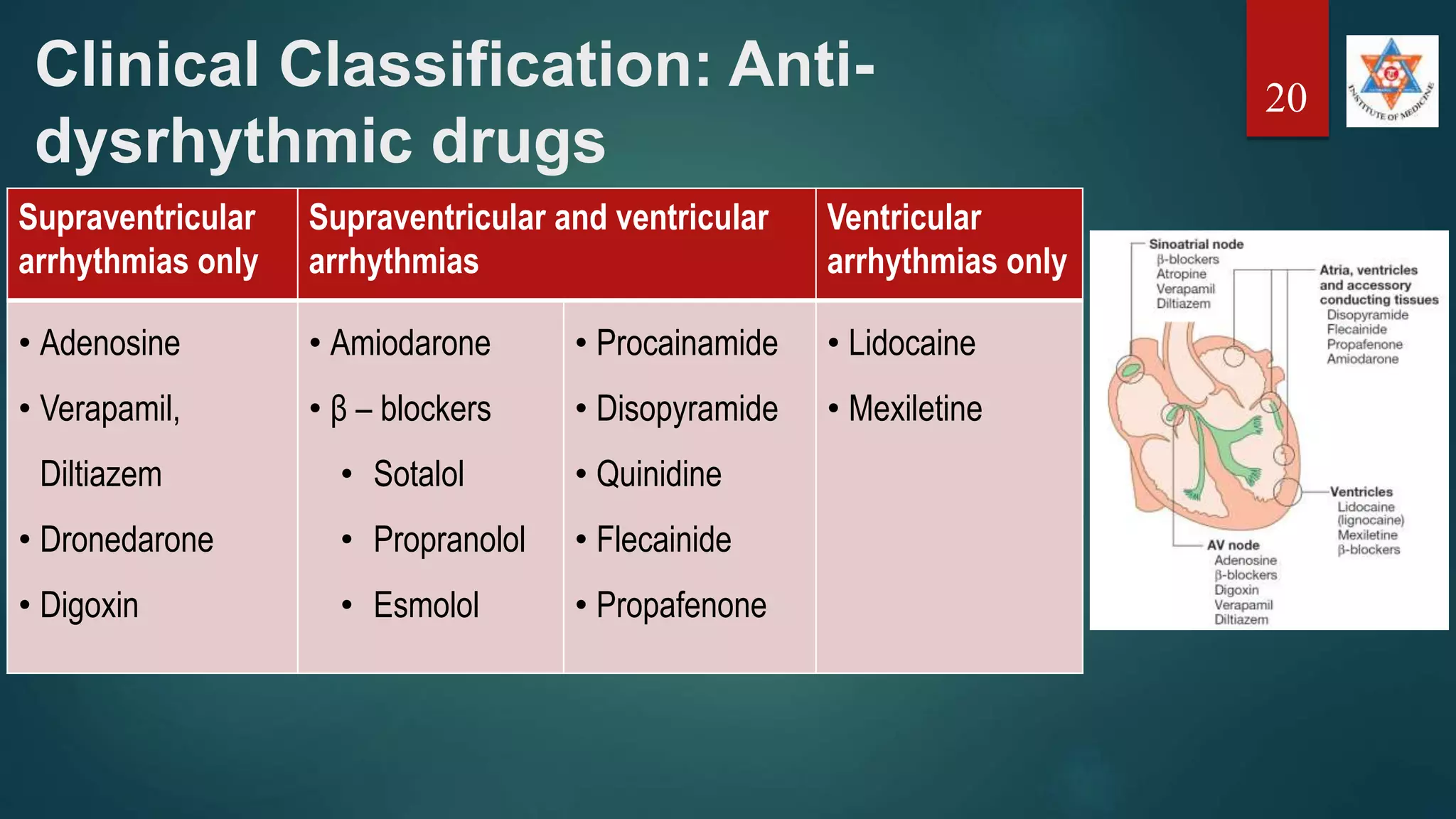
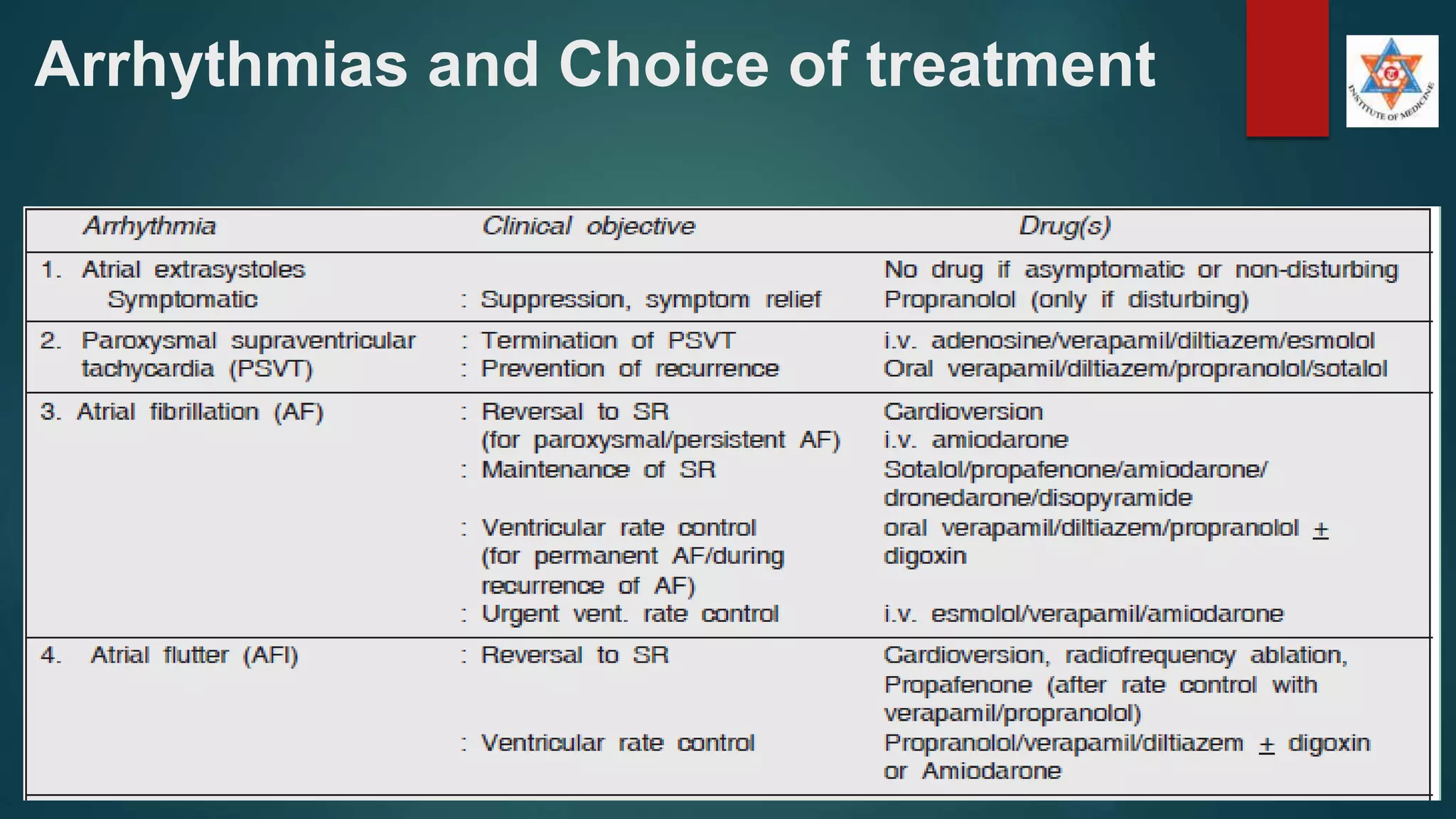


The document covers the topic of cardiac arrhythmias, providing definitions, mechanisms, clinical presentations, and treatment options, particularly pharmacotherapy. It emphasizes that arrhythmias can range from asymptomatic to life-threatening and highlights the importance of non-pharmacological treatment alongside drug therapy. The document also categorizes antiarrhythmic agents and discusses the drugs used for managing various types of arrhythmias.























































































