Drugs for heart failure
•Download as PPTX, PDF•
31 likes•7,291 views

This presentation deals with the use of various drugs in the treatment of heart failure such as Digoxin, ace inhibitors, beta bloockers, calcium channel blockers

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Drugs for heart failure
Similar to Drugs for heart failure (20)
More from Karun Kumar
More from Karun Kumar (20)
Recently uploaded
Recently uploaded (20)
Drugs for heart failure
- 1. Drugs for heart failure Dr. Karun Kumar JR – II Dept. of Pharmacology
- 6. Pathophysiology • End stage of CVD that impair the ability of ventricle • To fill with blood ; or • Eject blood into the circulation • Causes IHD (m/c), HTN, valvular disorders, arrhythmias, CMP, and constrictive pericarditis. • Less common Severe anaemia, B1 deficiency, or the use of certain anticancer drugs, such as doxorubicin, Transtuzumab
- 7. Cardiac or ventricular remodeling • characterized by 1.cardiac dilatation, 2.ventricular wall thinning, 3.interstitial fibrosis, 4.wall stiffness. • Impair the ability of the heart to relax or contract. 1. Activation of neuroendocrine systems (RAAS, SNS, inflammatory cytokines, local mediators [endothelin]) in response to myocardial ischemia Eg. angiotensin II induces collagen production and proliferation of fibroblasts. 2. Excessive stretch of muscle fibers
- 8. • Hallmark of HF ↓ SV & CO at any given diastolic muscle fiber length, by measuring the ventricular end diastolic pressure (preload). • ↓ stroke volume Due to 1. Diastolic dysfunction (Inability of the ventricles to fill properly) ↓ compliance (↑ stiffness) of ventricular tissue secondary to LVH/fibrosis 2. Systolic dysfunction (Inability of the ventricles to empty properly) Due to ↓ cardiac contractility secondary to a dilated or ischemic myocardium. • Both SHF/DHF caused by cardiac remodeling • LVF - LV does not adequately pump blood forward Pr. in pulm. Circul. ↑ Forces fluid into lung interstitium Congestion & edema
- 9. Pulmonary edema • ↓ diffusion of O2 & CO2 b/w alveoli & pulmonary capillaries Hypoxemia (deficient oxygenation of the blood) dyspnea (difficulty in breathing), including exertional dyspnea (dyspnea provoked by exercise), orthopnea (intensified dyspnea when lying flat), and paroxysmal nocturnal dyspnea (edema induced bronchoconstriction when sleeping)
- 11. • RVF – Cong. in peripheral veins ankle edema (ambulatory pt) & sacral edema(bedridden patient) • Also, hepatojugular reflux (↑ jugular vein distention when pressure is applied over liver) • RHF leads to LHF (LV forced to work harder for CO) . • ↓ CO Compensatory neuroendocrine responses (RAAS & SNS) which are counterproductive
- 12. • Both RAAS & SNS cause vascoconstriction • Arterial vc ↑ aortic impedance to LV ejection & ↓ CO • Angn II ADH,Ald.,cardiac remodeling & vent.wall thinning or fibrosis (↓ systolic & diastolic function) • Net result Further ↓ CO & ↑ circul. congestion
- 13. Drug therapy goals 1. Improve symptoms 2. Slow / reverse deterioration in myocardial func. 3. Prolong survival • Drugs can also be used to treat underlying conditions, control arrhythmias, prevent thrombosis, and treat anemia.
- 15. Drugs used for heart failure 1. ↑ CO (+ve inotropic drugs & vasodilators) 2. ↓ pulmonary & systemic congestion (Diuretics) 3. Slow or reverse cardiac remodeling (Ang & sym. Inh.) • Most significant dev. Ang. inhibitors, β blockers, • +ve inotropic drugs (Greek words for “fier” (inos) and “turning” or “to turn” (tropikos), the term inotropic refers to a change in muscle (fiber) contractility. (Digoxin, dobutamine, milrinone) [All 3 act by ↑ Calcium level in cardiac myocytes]
- 16. Digoxin • t1/2 36 hours (Elim. by renal excretion) • Narrow TI (Dose range 0.5 – 2 ng/ml) • +ve inotropic,-ve chronotr & -ve dromo effect • +ve Inotropic ↑ intracell Ca (inh. Na +,K+ATPase) • -ve chrono & dromo ↑ parasympathetic (vagal) tone & ↓ HR & AVN conduction velocity while ↑ AVN refractory period (slows rate in AF) • At the same time ↓ sympathetic tone (↓ vc)
- 20. Adverse Effects • GI, cardiac & neurologic reactions • Earliest signs of toxicity anorexia, N & V • Arrhythmias (most serious manifestation) AV block and various tachyarrhythmias. • Hypokalemia can precipitate arrhythmias in patients receiving digoxin • neurologic blurred vision and yellow, green, or blue chromatopsia (a condition in which objects appear unnaturally colored); seizures. • gynecomastia (estrogenic activity)
- 21. Interactions • Antacids and cholestyramine ↓ abs. of Digoxin • Diltiazem, quinidine & verapamil ↓ Digoxin clearance • Loop & thiazide diuretics hypokalemia (↓ K conc. ↑ digitalis binding to Na pump) • Hypokalemia can also contribute directly to arrhythmias
- 22. Indications • Syst. HF Inotropic effect & -ve chr., drom • NOT in diastolic HF contractility not impaired • HF + AF Most certain indication • Digoxin Immune Fab (i.v.( Igs from sheep immunized with a digoxin derivative.
- 23. Dobutamine (cont. i.v. infusion) • HF More freq. (selectively stimulates cardiac contractility & causes less tachycardia than other β- agonists) • Also activates β2 in vascular smooth muscle • Short term mx Acute HF & cardiogenic shock
- 24. Milrinone (Inodilator) • Inhibits type 3 PDE in heart & vasc. Sm. Musc. • Short term mx of HF, advanced HF & inotropic support of infants & children awaiting cardiac transplantation • Long term use Thrombocytopenia & ventricular arrhythmias and is associated with increased mortality in patients with severe heart failure
- 26. Vasodilators • angiotensin inhibitors, Hydral. + IDN, nesiritide • ↓ venous pressure (↓ edema) • ↓ arterial pressure (↓ cardiac afterload & ↑ CO) • Also, angiotensin inhibitors slow or reverse cardiac remodeling • ACE I DNephr, HTN & HF (counteract card. Rem.) • Ang II Vc, cardiac remodelling, ald., ADH • Ace i prevent the transition from asymptomatic to overt heart failure • Acute MI improve survival (within 24 hours) [prevents cardiac remodelling by Ang II]
- 27. Angiotensin Receptor Blockers • Do not inhibit bradykinin degradation and are not prone to induce chronic cough • As effective as ACE inhibitors in treating heart failure. • Indic. pts. who cannot tolerate ACE inhibitor. • Valsartan, Candesartan
- 28. Hydralazine and Nitrates • IDN Relaxes venous smooth muscle, • Hydralazine relaxes arterial smooth muscle • combined use ↓ cardiac preload (↓ venous pressure and edema) & afterload (↑ CO) • pts with HF who cannot tolerate an angiotensin inhibitor.
- 29. Nesiritide (only i.v.) • human B-type NP from E. coli using rDNA • T/t of patients with acutely decompensated heart failure who have shortness of breath (dyspnea) at rest or with minimal activity. • Nesiritide binds to g.c. receptor in vascular smooth muscle and endothelial cells ↑ cGMP dilate venous and arterial smooth muscle • A/E hypotension
- 30. PCWP
- 31. β-blockers • Exc. SNS Cardiac remodeling by :- 1. Tachycardia (β1 receptors) ↑ MOD 2. RAAS 3. Chr. Stim. of cardiac β rec. myocyte hypertrophy & apoptosis Cardiac dilatation & ventricular wall thinning 4. ↑ cardiac cytokines (TNF α & Ils) induce myocyte hypertrophy and apoptosis Fibrosis & ventricular wall stiffness. • β bl. ↓ exc. Sympath. Stimul. of heart (Mild to severe HF caused by LV systolic dysfunction) •
- 32. • Carvedilol β1,β2, α1 (vd); antioxidant, antiinflmmatory and antiapoptotic (multiple-action neuroendocrine antagonist). • Given in symptomatic HF without hypotension, pulmonary congestion, or AV block. • A/E Bradycardia, worsening heart failure, and dizziness or light headedness (vd & ↓ BP) • Started on low doses & then gradually ↑ (beneficial effects have a delayed onset of action & a/e occur immediately) • Also, can lead to ↑ symptoms for 4 to 10 weeks before any improvement is noted
- 33. Aldosterone antagonists • Prev. A/E of exc. Ald. on heart • patients should be monitored closely (hyperkal.) • Spironolactone produces endocrine side effects resulting from its binding to androgen and progesterone receptors and leading to gynecomastia and impotence in some male patients. • Eplerenone produces fewer endocrine side effects than spironolactone
- 34. Diuretics • HF - ↓ plasma volume & edema Relieve symptoms of volume overload (dyspnea) • Loop diuretics are preferred but must be used carefully to avoid dehydration, hyponatremia, and hypokalemia • Hypokalemia ↑ risk of digoxin toxicity • Thiazide diuretics used when a lesser degree of diuresis is required
- 35. Management of heart failure • Goals of therapy 1. Relieve symptoms 2. improve quality of life 3. prolong survival. • Acute HF Hospitalization & i.v. vasodilators (NO3 & Nesiritide), diuretics, inotropic agents, & O2 • Once stabilized Oral medications, dietary restrictions, & exercise guidelines • Bed rest early course of therapy • Incremental exercise program After improving
- 36. Management of chronic HF • Depends on 1. underlying cause 2. degree of cardiac dysfunction 3. Signs & symptoms exhibited by patient • Systolic HF ACE i.+ BB + loop diur. + ald. Antag. • Some patients benefit by addition of digoxin &/or combination of hydralazine and a nitrate, whereas anticoagulant and antiplatelet drugs may be needed by some patients. • ARBs Cannot tolerate an ACE inhibitor.
Editor's Notes
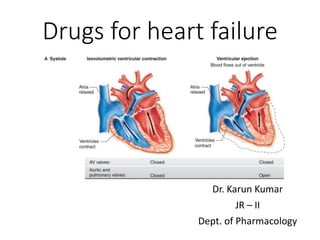
- At the start of ventricular systole, the AV valves close. Ventricular muscle initially shortens relatively little, but intraventricular pressure rises sharply as the myocardium presses on the blood in the ventricle ( Figure 30–2 ). This period of isovolumetric (isovolumic, isometric) ventricular contraction lasts about 0.05 s, until the pressures in the left and right ventricles exceed the pressures in the aorta (80 mm Hg; 10.6 kPa) and pulmonary artery (10 mm Hg) and the aortic and pulmonary valves open. During isovolumetric contraction, the AV valves bulge into the atria, causing a small but sharp rise in atrial pressure (Figure 30–3 ). When the aortic and pulmonary valves open, the phase of ventricular ejection begins. Ejection is rapid at first, slowing down as systole progresses. The intraventricular pressure rises to a maximum and then declines somewhat before ventricular systole ends. Peak pressures in the left and right ventricles are about 120 and 25 mm Hg, respectively. Late in systole, pressure in the aorta actually exceeds that in the left ventricle, but for a short period momentum keeps the blood moving forward. The AV valves are pulled down by the contractions of the ventricular muscle, and atrial pressure drops. The amount of blood ejected by each ventricle per stroke at rest is 70–90 mL. The end-diastolic ventricular volume is about 130 mL. Thus, about 50 mL of blood remains in each ventricle at the end of systole(end-systolic ventricular volume) ,and the ejection fraction , the percentage of the end-diastolic ventricular volume that is ejected with each stroke, is about 65%. The ejection fraction is a valuable index of ventricular function. It can be measured by injecting radionuclide-labelled red blood cells and imaging the cardiac blood pool at the end of diastole and the end of systole (equilibrium radionuclide angiocardiography), or by computed tomography. MAP=CO X TPR (syst. Art. Press.)
- pathophysiology of heart failure with reduced ejection fraction (HF‐reF) and drug targeting mechanisms. as illustrated, HF is typically initiated by a primary myocardial injury, most commonly myocardial infarction (MI). This injury results in left ventricular dysfunction and decreased cardiac output (CO). The reduced CO in turn sets off an initially compensatory response and subsequently progressive maladaptation, leading to myocardial remodeling and deterioration of left ventricular dysfunction. This vicious cycle is perpetuated primarily via sustained activation of the renin–angiotensin–aldosterone system (raaS) and the sympathetic nervous system (SnS). drugs that target the raaS and SnS retard cardiac remodeling and slow disease progression, and as such, have become the cornerstone of HF management. diuretics, vasodilators, and positive inotropic agents act at various steps of the HF pathophysiology to improve symptoms associated with left ventricular dysfunction. On the other hand, cardiac‐resynchronization therapy (CrT) improves left ventricular function via correcting the conduction abnormalities. raaSIs denotes raaS inhibitors, which include angiotensin‐converting enzyme inhibitors, angiotensin receptor blockers, and aldosterone receptor antagonists. LVeF denotes left ventricular ejection fraction.
- T romboxane A2 promotes platelet aggregation and vasoconstriction, whereas prostacyclin inhibits platelet aggregation and promotes vasodilation.
- Arterial blood pressure The force exerted by the blood against any unit area of the arterial vessel wall.
- 2. excessive stretch of muscle fibersFor
- Mechanisms by which digoxin exerts its positive inotropic effect on the heart. Digoxin inhibits the sodium pump (ATPase) in the sarcolemma and increases the concentration of intracellular sodium. The high sodium concentration increases the activity of the sodium calcium exchanger (Ex), thereby causing more calcium to enter or remain inside the cardiac myocyte. Calcium activates muscle fier shortening and increases cardiac contractility, which in turn increases stroke volume at any given fiber length (preload). Starling pointed this out when he stated that the “energy of contraction is proportional to the initial length of the cardiac muscle fiber” (Starling’s law of the heart or theFrank–Starling law ). For the heart, the length of the muscle fibers (ie, the extent of the preload) is proportional to the end-diastolic volume. The relation between ventricular stroke volume and end-diastolic volume is called the Frank–Starling curve.
- Electrophysiologic and electrocardiographic effects of digoxin. Digoxin causes an increase in parasympathetic (vagal) tone and a decrease in sympathetic tone. These actions slow the heart rate by decreasing sinoatrial (SA) node automaticity. The increased vagal tone and decreased sympathetic tone also slow the atrioventricular (AV) node conduction velocity while increasing the AV node refractory period. The reduced AV conduction velocity increases the PR interval on the electrocardiogram. In ventricular tissue, digoxin shortens the action potential duration, and this decreases the QT interval. Toxic concentrations of digoxin may evoke afterdepolarizations throughout the heart and thereby cause extrasystoles and tachycardia. Digoxin also causes STsegment depression, which gives rise to the socalled “hockey stick confiuration” on the electrocardiogram. extrasystoles (premature or coupled beats) and tachycardia (rapid beating of the heart). The afterdepolarizations appear to be caused by excessive calcium inflx into cardiac cells, and they are more likely to occur after higher doses of digoxin have been given
- Pulmonary capillary wedge pressure (PCWP) provides an indirect estimate of left atrial pressure (LAP). Although left ventricular pressure can be directly measured by placing a catheter within the left ventricle, it is not feasible to advance this catheter back into the left atrium. LAP can be measured by placing a special catheter into the right atrium then punching through the interatrial septum; however, for obvious reasons, this is not usually performed because of damage to the septum and potential harm to the patient. PCWP is measured by inserting balloon-tipped, multi-lumen catheter (Swan-Ganz catheter) into a peripheral vein, then advancing the catheter into the right atrium, right ventricle, pulmonary artery, and then into a branch of the pulmonary artery. Just behind the tip of the catheter is a small balloon that can be inflated with air (~1 cc). The catheter has one opening (port) at the tip (distal to the balloon) and a second port several centimeters proximal to the balloon. These ports are connected to pressure transducers. When properly positioned in a branch of the pulmonary artery, the distal port measures pulmonary artery pressure (~ 25/10 mmHg; systolic/diastolic pressure) and the proximal port measures right atrial pressure (~ 0-3 mmHg). The balloon is then inflated, which occludes the branch of the pulmonary artery. When this occurs, the pressure in the distal port rapidly falls, and after several seconds, reaches a stable lower value that is very similar to left atrial pressure (normally about 8-10 mmHg). The balloon is then deflated. The same catheter can be used to measure cardiac output by the thermodilution technique. The pressure recorded during balloon inflation is similar to left atrial pressure because the occluded vessel and its distal branches that eventually form the pulmonary veins act as a long catheter that measures the blood pressures within the pulmonary veins and left atrium. Why is it measured? It is helpful to measure PCWP to diagnose the severity of left ventricular failure and to quantify the degree of mitral valve stenosis. Both of these conditions elevate LAP and therefore PCWP. These pressures are normally 8-10 mmHg. Aortic valve stenosis and regurgitation, and mitral regurgitation also elevate LAP. When these pressures are above 20 mmHg, pulmonary edema is likely to be present, which is a life-threatening condition. Note that LAP is the outflow or venous pressure for the pulmonary circulation and increases in LAP are transmitted almost fully back to the pulmonary capillaries thereby increasing their hydrostatic pressure and filtration of fluid. By measuring PCWP, the physician can titrate the dose of diuretic drugs and other drugs that are used to reduce pulmonary venous and capillary pressure, and thereby reduce pulmonary edema. Therefore, measurement of PCWP can help guide therapeutic efficacy. PCWP is also important to measure when evaluating pulmonary hypertension. Pulmonary hypertension is often caused by increased pulmonary vascular resistance. To calculate this, pulmonary blood flow (usually measured by the thermodilution technique), pulmonary artery pressure and pulmonary venous pressure (PCWP) measurements are required. Pulmonary hypertension can also result from increases in pulmonary venous pressure and pulmonary blood volume secondary to left ventricular failure or mitral or aortic valve disease. PCWP is also useful in evaluating blood volume status when fluids are administered during hypotensive shock. One practice is to administer fluids at a rate that maintains PCWP between 12-14 mmHg.
- Metoprolol and bisoprolol have also been shown to produce benefiial effects in patients with heart failure. Some studies, however, suggest that these drugs are not as benefiial as carvedilol in some patients with heart failure. In the Carvedilol or Metoprolol European Trial (COMET). of patients with heart failure, carvedilol reduced mortality more than did metoprolol. This study has been criticized with respect to whether the doses of the βblockers used in the study produced the same degree of βblockade.