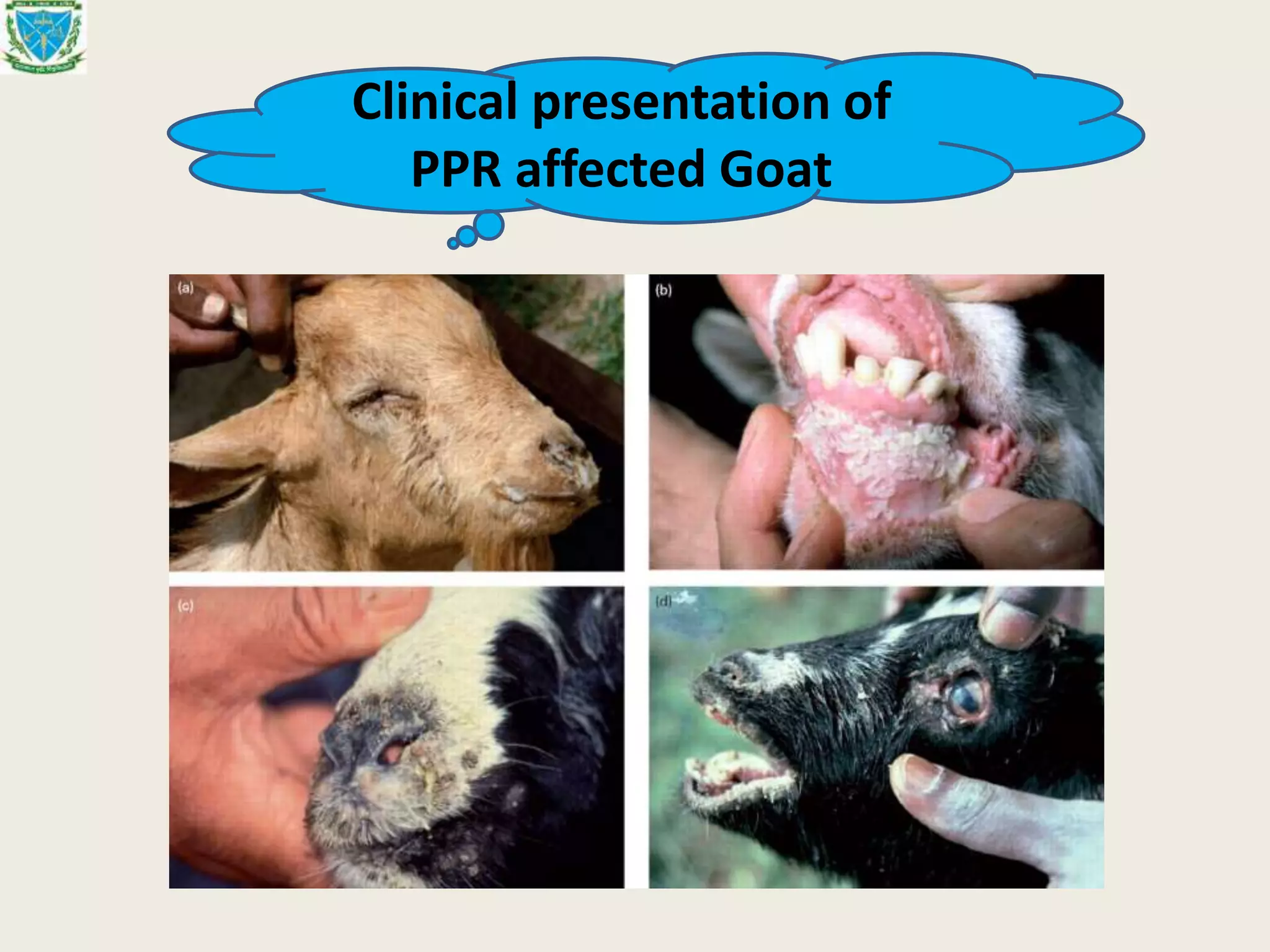
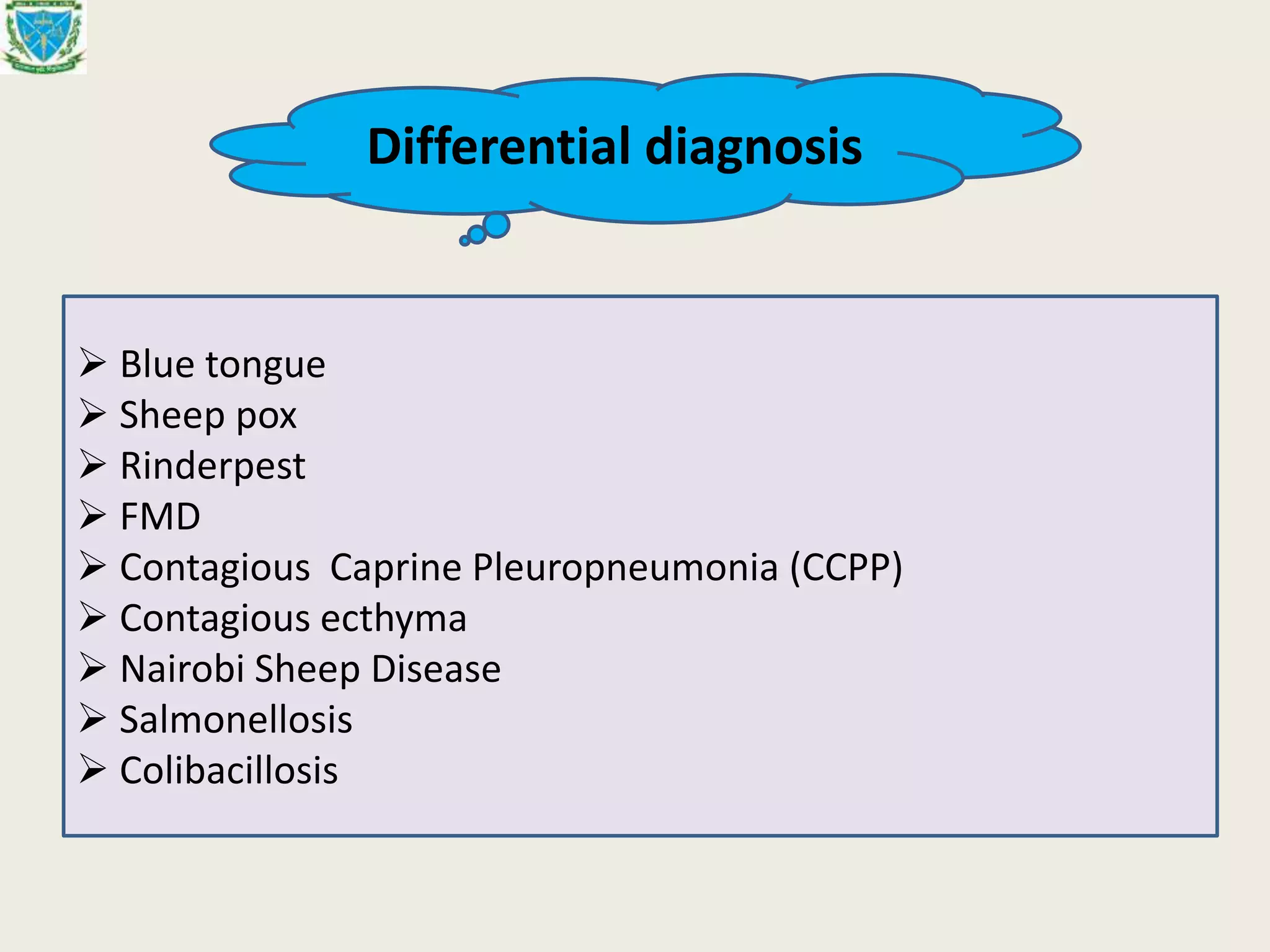
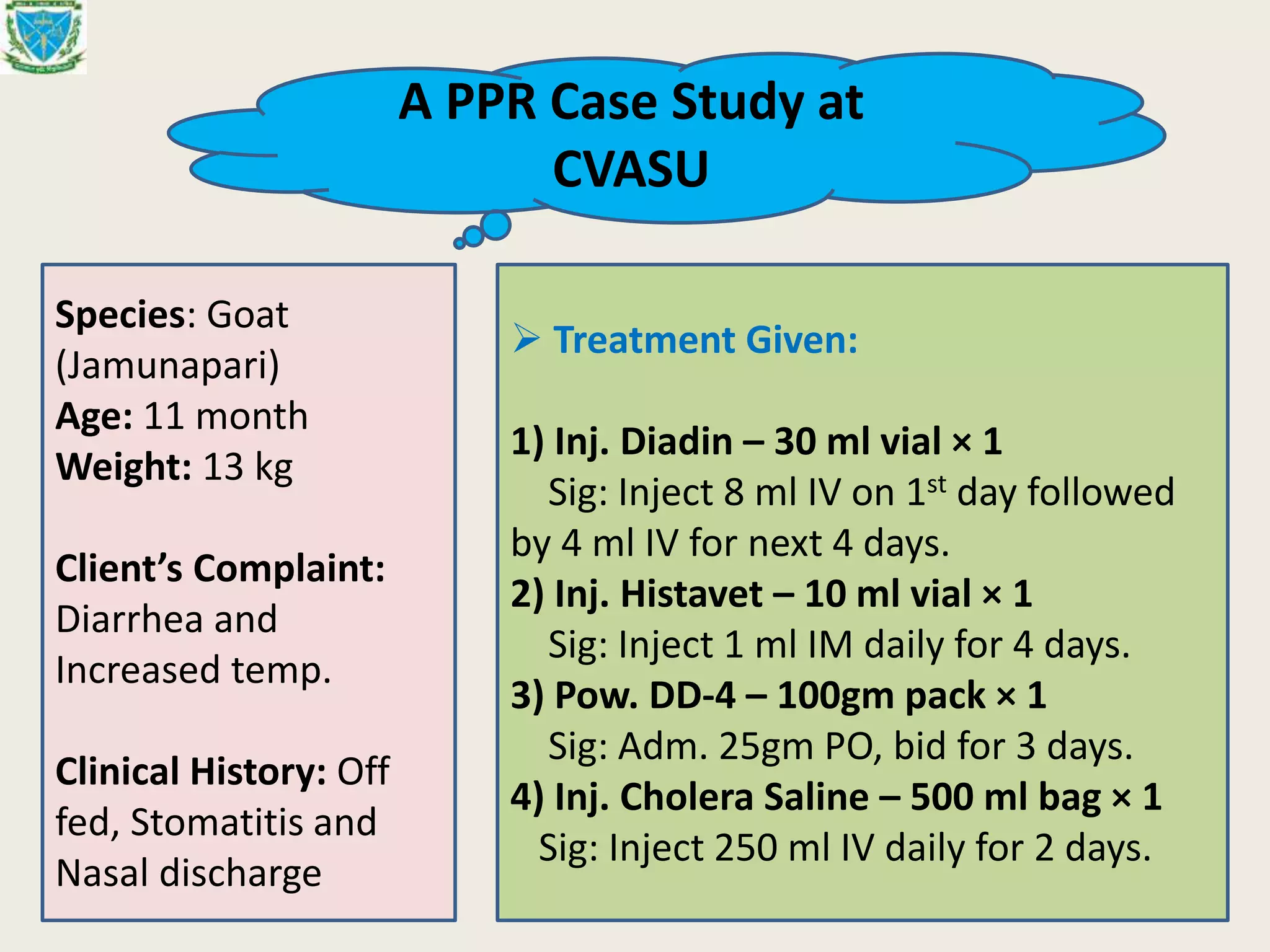
The document provides a comprehensive overview of Peste des Petits Ruminants (PPR), an acute, highly contagious viral disease affecting goats and sheep, characterized by severe symptoms, high morbidity, and mortality rates. It discusses the disease's origin, economic impact, transmission methods, clinical manifestations, diagnosis, treatment options, and prevention strategies including vaccination methods. The document emphasizes the importance of control measures and the global effort launched in 2015 by FAO and OIE to manage PPR outbreaks.