Download as PDF, PPTX
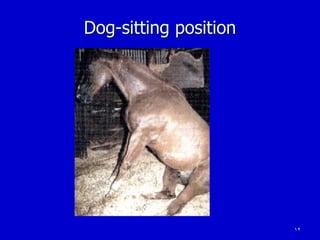
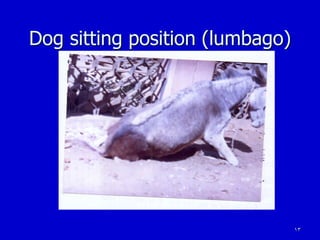
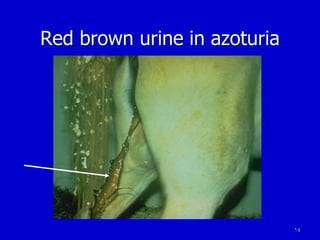
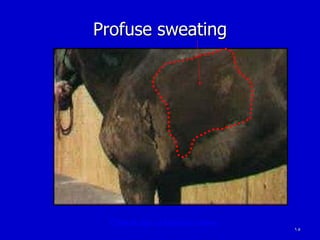


Azoturia, also known as Monday morning disease or tying-up syndrome, is a metabolic muscular disorder in horses characterized by stiffness, lameness, and muscle swelling. It occurs after a period of at least 2 days rest when horses return to exercise on a full ration. The major cause is carbohydrate overloading from excessive glycogen buildup in muscles during rest, leading to lactic acid accumulation during subsequent exercise and muscle damage. Clinical signs range from poor performance to an inability to rise. Diagnosis involves detecting myoglobin in the urine and elevated muscle enzyme levels in blood. Treatment focuses on rest, pain relief, intravenous fluids, and thiamine supplementation.























































































