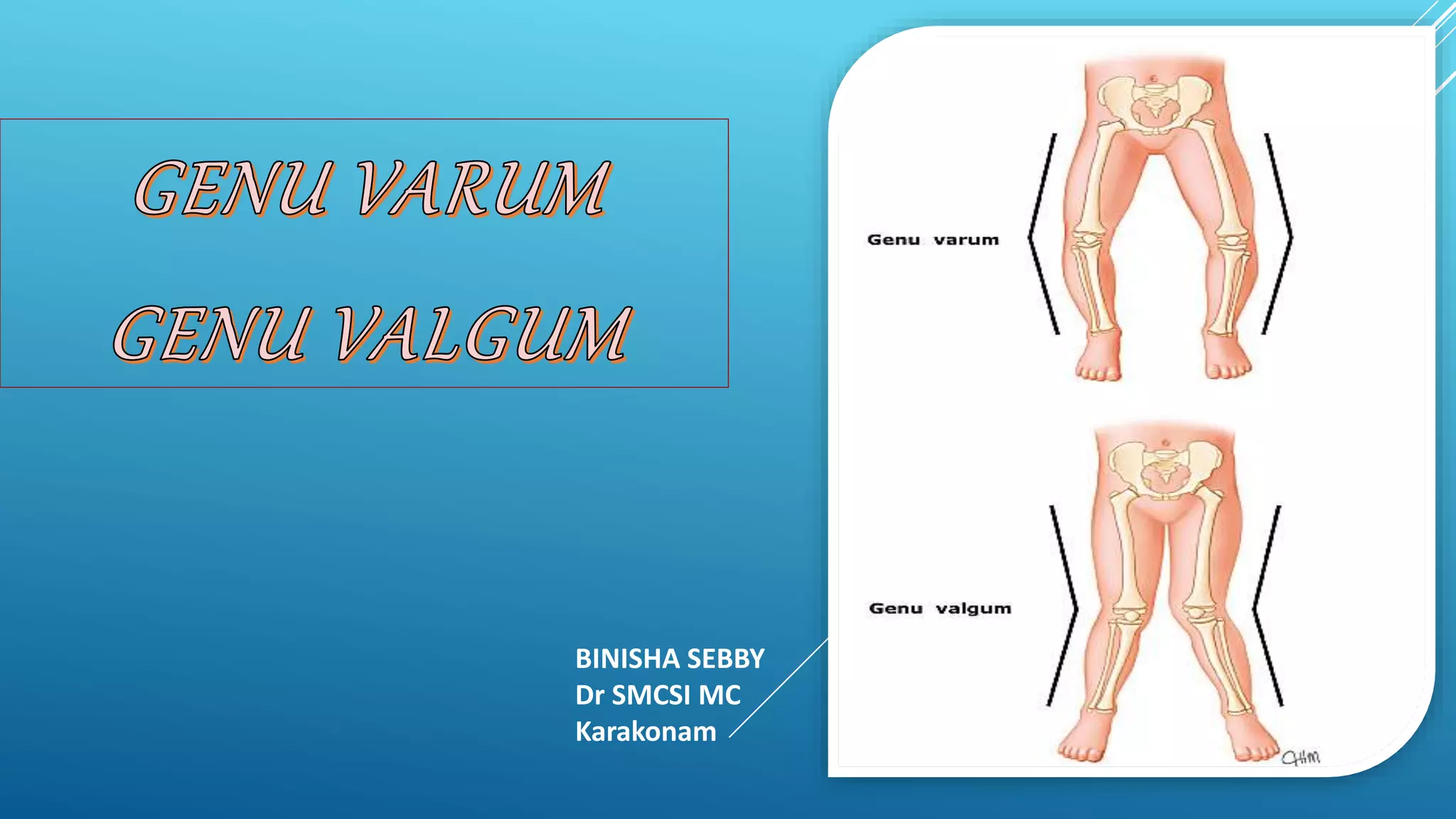
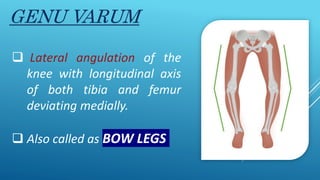
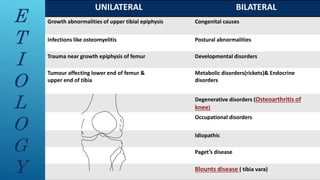
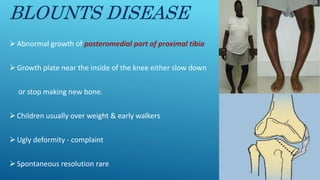
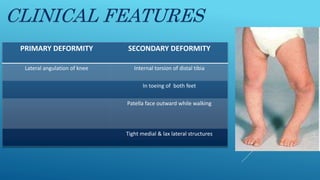
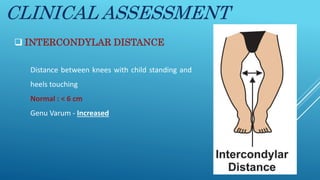
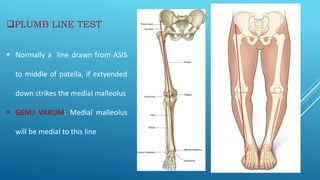
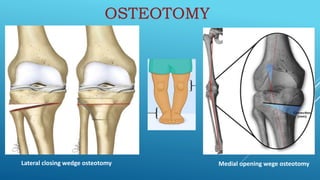
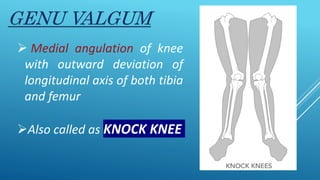
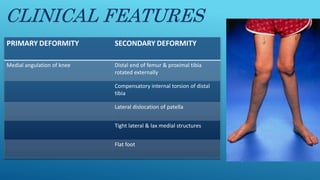
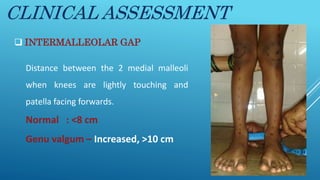
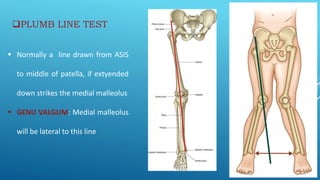
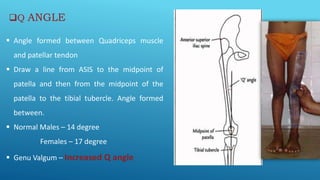
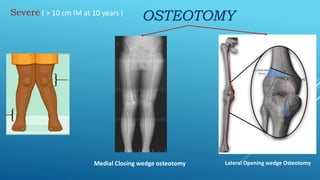
This document discusses genu varum (bow legs) and genu valgum (knock knees) in children. Genu varum is caused by lateral angulation of the knee with the femur and tibia deviating medially, while genu valgum involves medial angulation with outward deviation. Clinical features, assessment methods like the intercondylar/intermalleolar distance and plumb line tests, and treatment options like epiphyseal stapling and osteotomies are described for both conditions. Blount's disease, which causes abnormal proximal tibial growth, is also summarized.