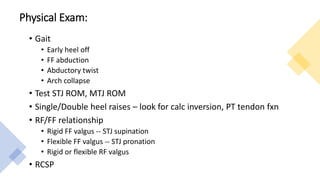
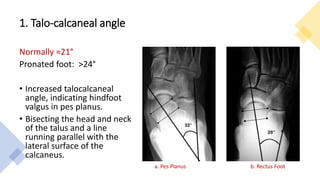
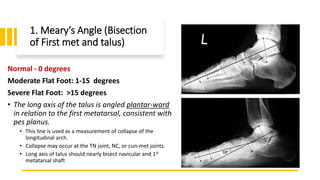
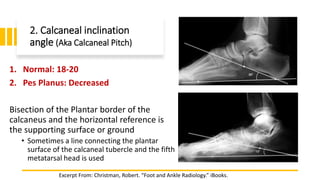
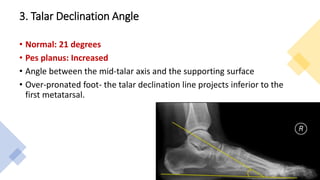
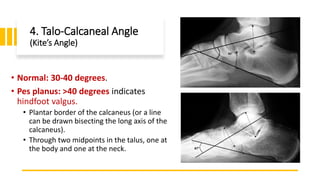
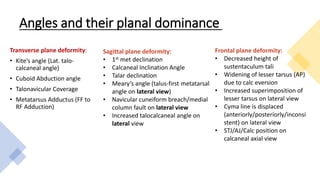
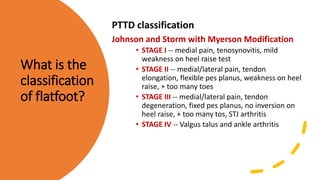
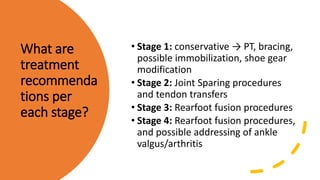
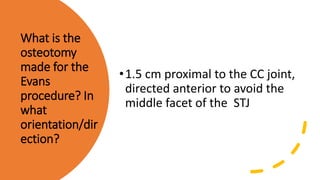
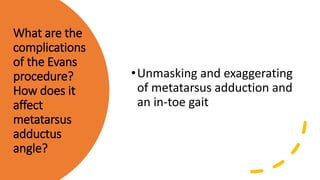
The document provides guidance on how to effectively work up and summarize a surgical patient case during a residency interview. It emphasizes knowing the preferred procedures of the interviewing program and being able to describe radiographic findings of flat feet in a systematic way. For a flat foot work up, the assistant should identify deformities in the sagittal, frontal, and transverse planes, then suggest procedures to address each, such as a gastrocnemius recession for sagittal plane correction or a medial calcaneal slide for frontal plane correction. Reading flat foot radiographs involves assessing specific angles on both AP and lateral views that indicate planovalgus deformity severity and type.




![Additional Reading:
[Hix J, et al. Calcaneal osteotomies for the treatment of adult-acquired flatfoot. Clin Podiatr Med Surg.
2007 Oct; 24(4): 699-719.]
[Mosier-LaClair S, et al. Operative treatment of the difficult stage 2 adult acquired flatfoot deformity.
Foot Ankle Clin. 2001 Mar; 6(1): 95-119.]
[Roye DP, Raimondo RA. Surgical treatment of the child’s and adolescent’s flexible flatfoot. Clin
Podiatr Med Surg. 2000 Jul; 17(3): 515-30.]
[Toolan BC, Sangeorzan, Hansen. Complex reconstruction for the treatment of dorsolateral peritalar
subluxation of the foot. JBJS-Am. 1999 Nov; 81(11): 1545-60.]
[Weinraub GM, Heilala MA. Adult flatfoot/posterior tibial tendon dysfunction: outcomes analysis of
surgical treatment utilizing an algorithmic approach. J Foot Ankle Surg. 2001 Jan-Feb; 40(1): 54-7.]](https://image.slidesharecdn.com/flatfootwork-up-200514111344/85/Flat-foot-work-up-59-320.jpg)



































![flat foot.ppt [pes planus ] #physio.# rehabilitation](https://cdn.slidesharecdn.com/ss_thumbnails/flatfoot-240310065759-517e9bef-thumbnail.jpg?width=640&height=640&fit=bounds)



















































