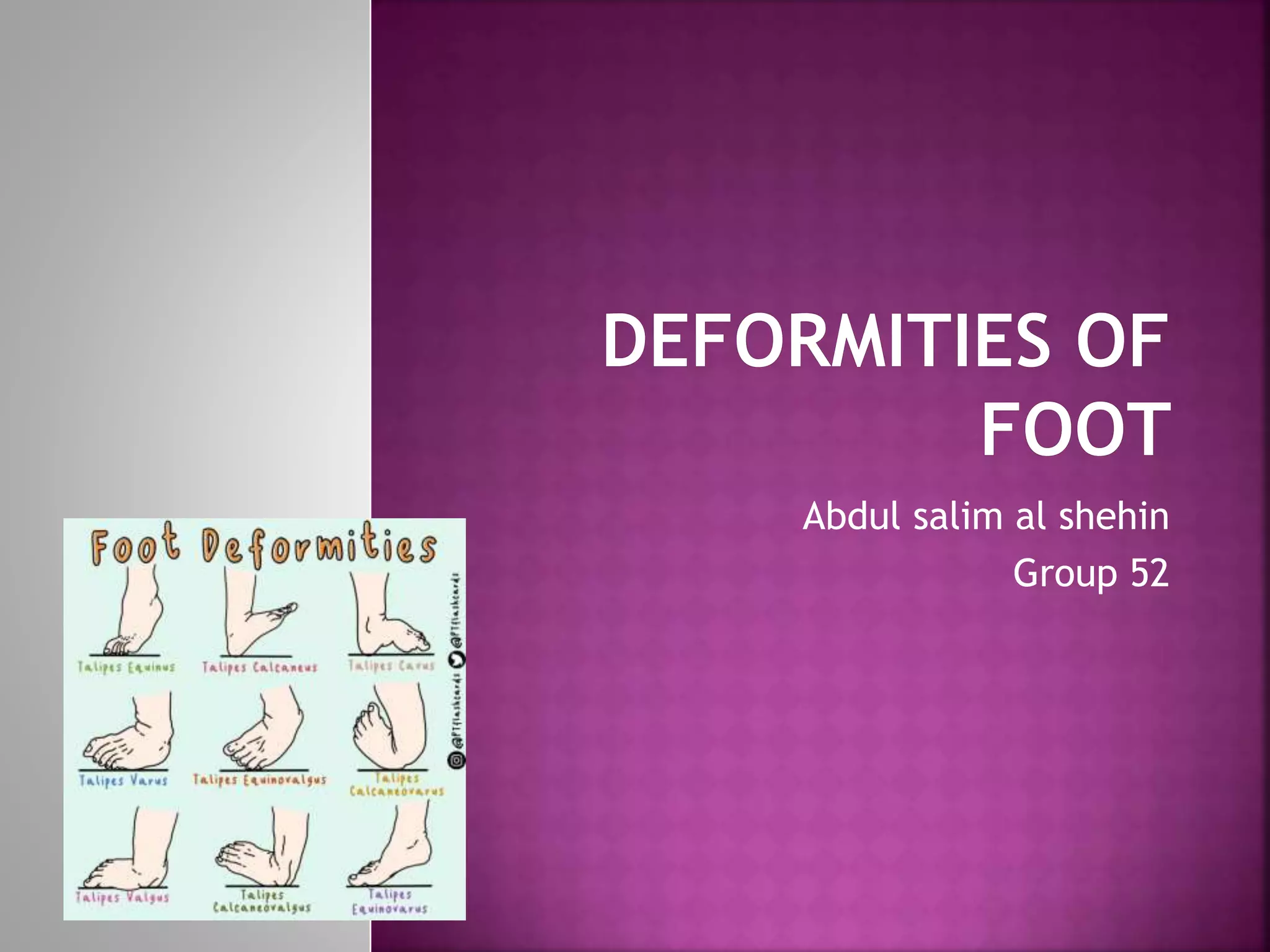
This document discusses several types of foot deformities:
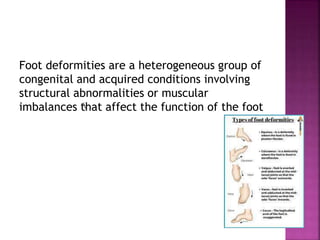
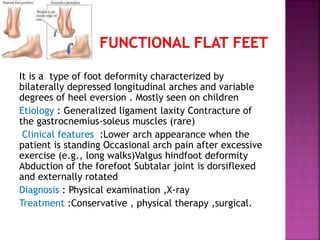
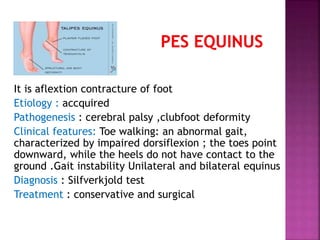
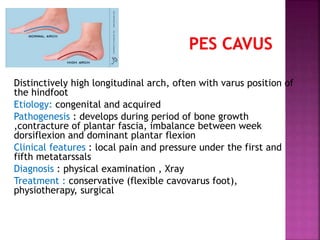
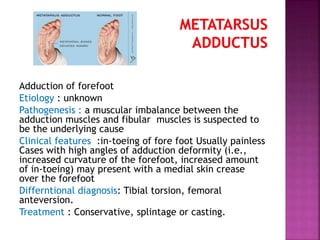
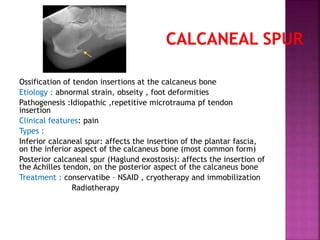
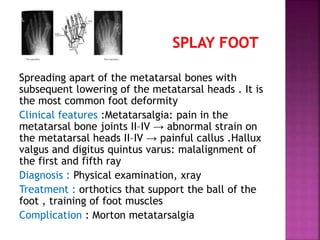
Pes planus (flat feet) is a rare deformity involving structural abnormalities of the talus and subtalar joints. Equinus is a flexion contracture of the foot that can cause toe walking. Cavovarus foot has a high longitudinal arch and varus hindfoot positioning. Hallux valgus involves adduction of the forefoot. Calcaneal spurs form at the insertion of the plantar fascia and Achilles tendon. Metatarsus adductus is the adduction of the forefoot. Morton's toe is a spreading of the metatarsal bones causing calluses.