Downloaded 518 times










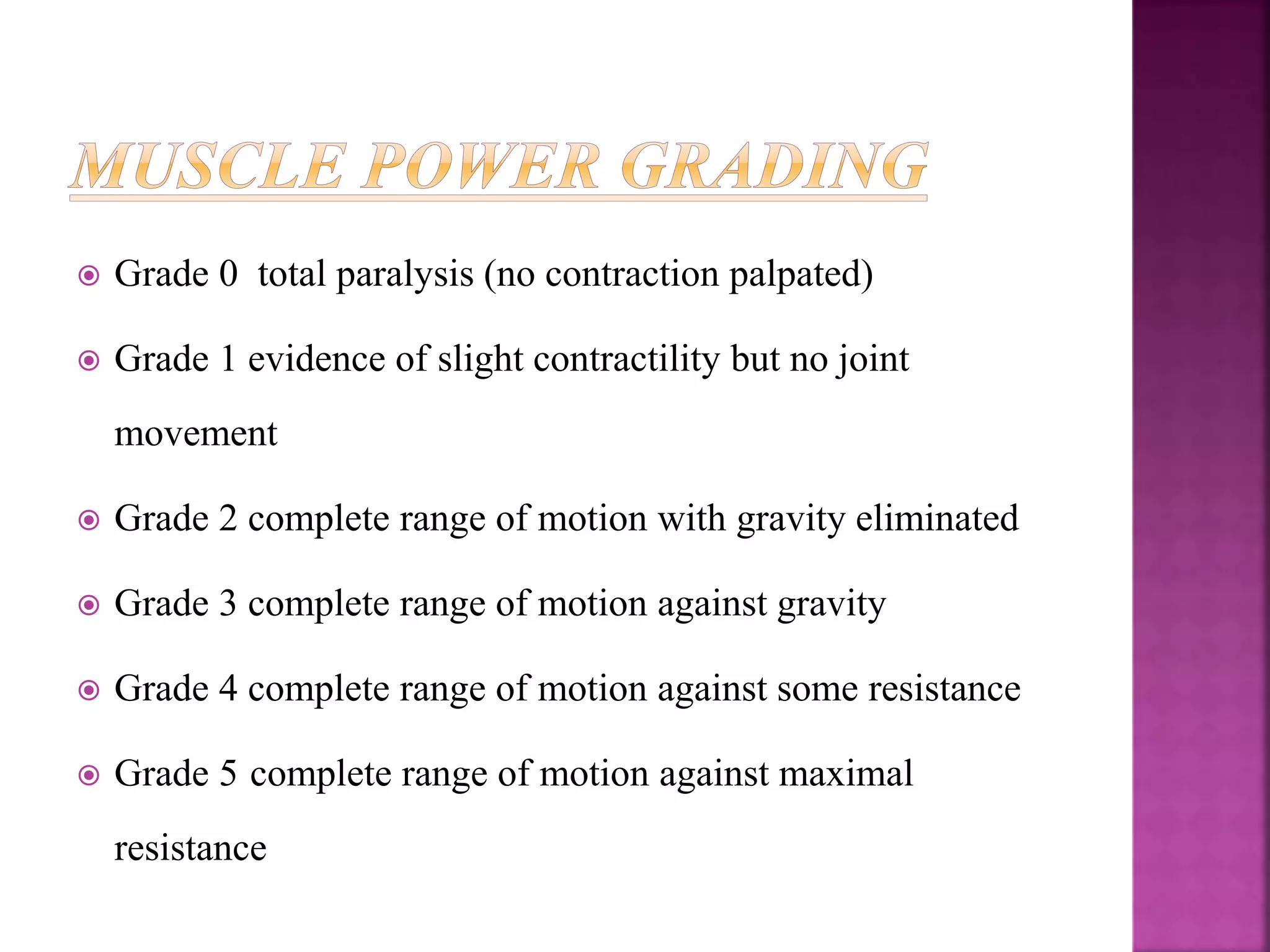



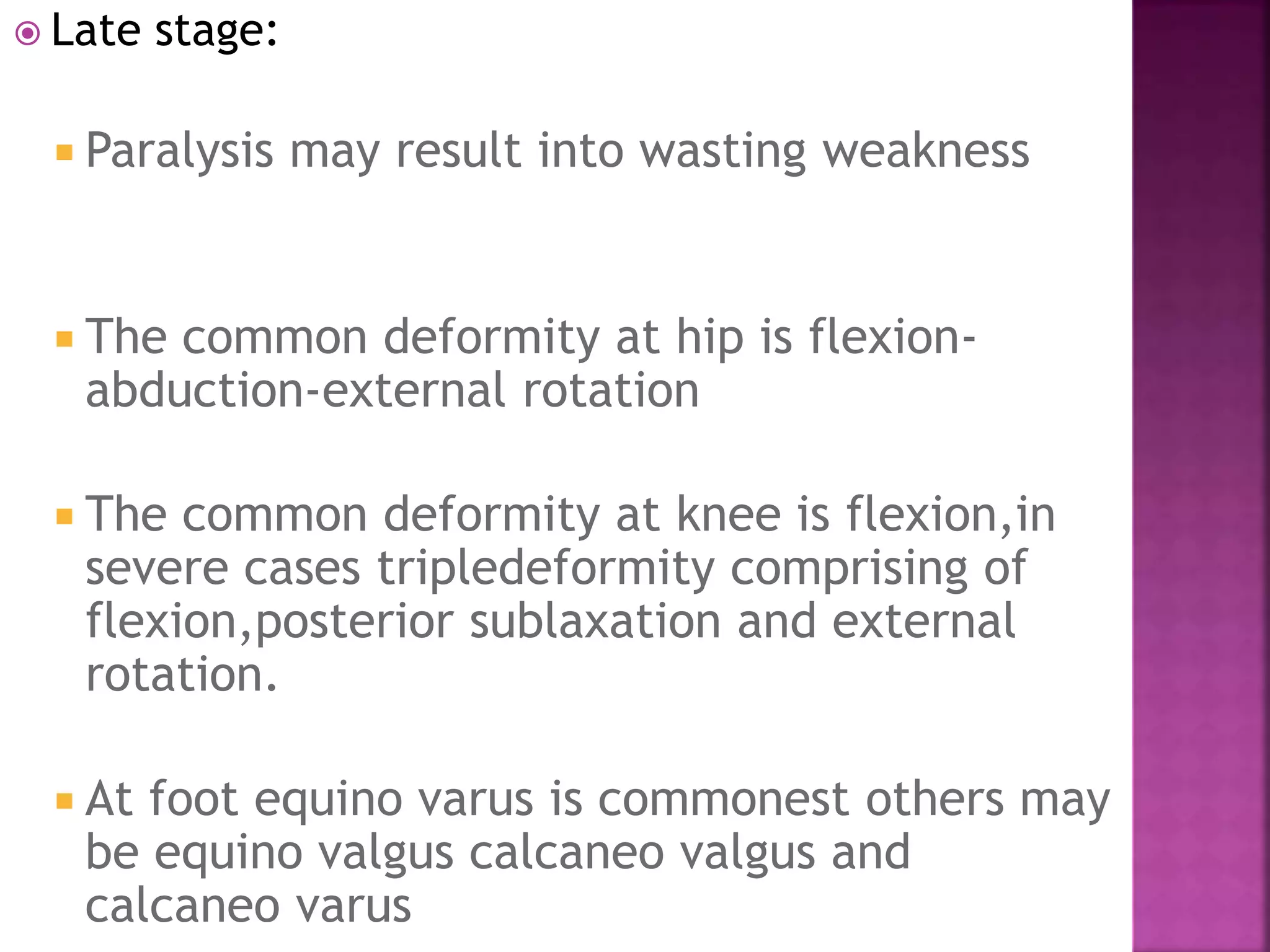

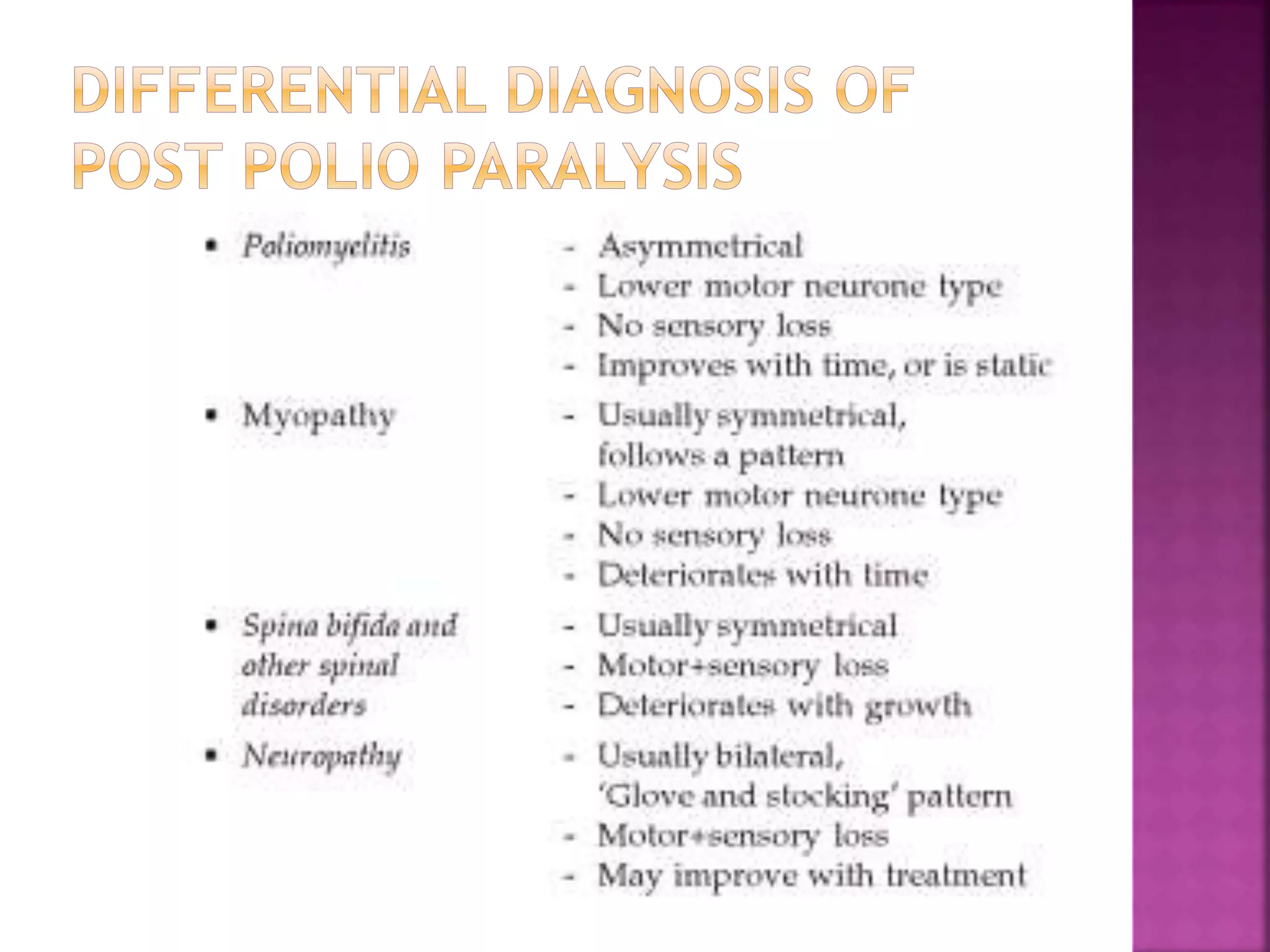












































This document discusses poliomyelitis (polio), including its clinical manifestations, stages, and common muscle involvement. It then focuses on the causes and management of progressive deformities that can result from polio, such as muscle imbalance, unreleived muscle spasm, growth issues, gravity, and posture. Specific deformities at the hip, knee, ankle, and foot are described. The management of polio involves addressing these deformities through reconstructive surgery, physiotherapy, orthotics, tendon transfers, and arthrodesis.



































































