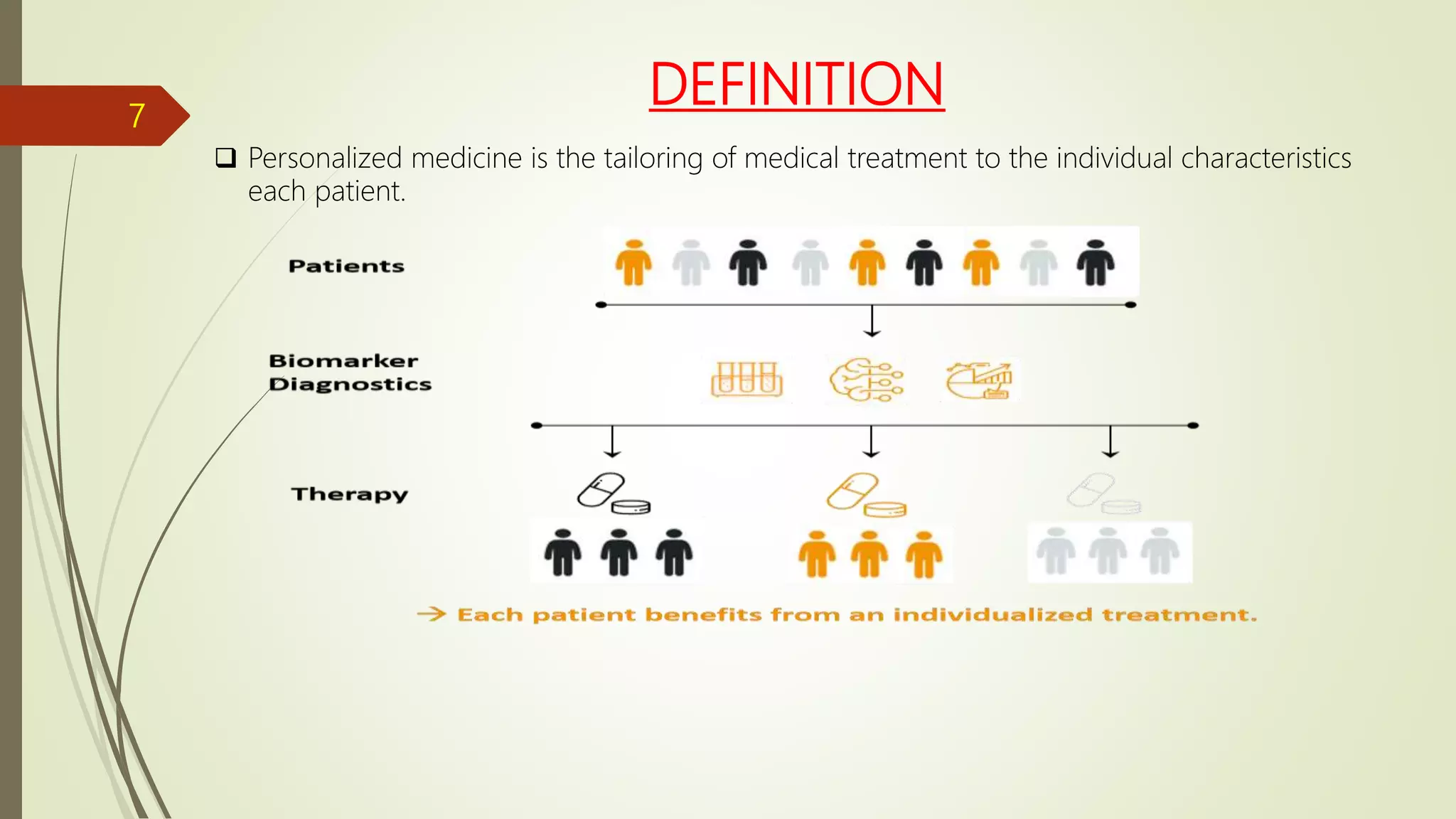
This document discusses personalized medicine and pharmacogenetics. It defines personalized medicine as tailoring medical treatment to an individual's characteristics. Pharmacogenetics is the study of how genetic differences influence variability in drug responses. The document outlines how genetic polymorphisms can impact drug metabolism and efficacy through variations in phase I and phase II drug metabolizing enzymes. It also categorizes different types of patients who may benefit from personalized medicine approaches based on factors like age, gender, medical conditions, and genetics.