Pharmacogenetics and
Personalized Therapy:
AdvancingDrug
Therapy
Welcome to this presentation exploring the exciting field of
pharmacogenetics and its impact on personalized therapy. We'll
delve into the science behind how genes influence drug
responses, explore the promises and challenges of this
transformative approach to medicine, and showcase real-world
examples of its success.
Presented by:
Omer Muhammed Asaad
Supervised by:
Assit. Prof. Nidhal Muhammed Ali
2.
Outlines:
• Introduction toPharmacogenetics
• The Promise of Personalized Medicine
• Pharmacogenetics vs. Pharmacogenomics
• The Pharmacogenomics Knowledge Base (PharmGKB)
• Individual variations
• Key Genes in Drug Metabolism
• CYP2D6 and Drug Metabolism
• CYP2C9 and Drug Metabolism
• CYP2C19 and Drug Metabolism
• GENETIC VARIATION
• Integrating Pharmacogenetics into Clinical applications
• The Future of Medicine
Introduction to Pharmacogenetics
•The Genetic Testing Registry (GTR)
in the United States accepts
submissions from laboratories
worldwide regarding the genetic
tests that are made available for
the purposes of screening,
diagnosis, drug/disease
monitoring and treatment
response.
5.
Introduction to Pharmacogenetics
•Pharmacogenomics can play an important role in identifying
responders and non-responders to medications, avoiding
adverse events, and optimizing drug dose. Drug labeling may
contain information on genomic biomarkers and can describe:
• Drug exposure and clinical response variability
• Risk for adverse events
• Genotype-specific dosing
• Polymorphic drug target and disposition genes
6.
The Promise ofPersonalized
Medicine: Matching Therapies
to Genotypes
Personalized medicine holds the
promise of revolutionizing
healthcare by tailoring treatment
plans based on each patient's
unique genetic makeup. This
approach moves away from a
one-size-fits-all strategy, aiming
to improve drug efficacy and
safety while minimizing adverse
effects.
By understanding an individual's
genetic profile, doctors can
select the most appropriate
medications and adjust doses to
optimize therapeutic outcomes.
This personalized approach aims
to increase the likelihood of
successful treatment while
minimizing side effects and drug
interactions.
Furthermore, personalized medicine has the potential to reduce
healthcare costs by preventing unnecessary hospitalizations and
complications associated with ineffective or poorly tolerated medications.
7.
The Promise ofPersonalized Medicine
• Shifting from "one-size-fits-all" to tailored treatments.
• Reducing adverse drug reactions and improving efficacy.
• Genes influence pharmacokinetics by altering drug ADME-related proteins.
• Genes influence pharmacodynamics through variations in drug targets: G
proteins or other downstream pathways.
• Genetic differences also contribute to rare adverse reactions.
• Genetic information may soon enable precise drug selection, ensuring
efficacy and safety while reducing trial-and-error prescribing—an
approach known as personalized medicine.
8.
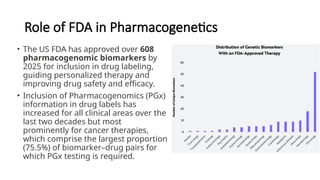
Role of FDAin Pharmacogenetics
• The US FDA has approved over 608
pharmacogenomic biomarkers by
2025 for inclusion in drug labeling,
guiding personalized therapy and
improving drug safety and efficacy.
• Inclusion of Pharmacogenomics (PGx)
information in drug labels has
increased for all clinical areas over the
last two decades but most
prominently for cancer therapies,
which comprise the largest proportion
(75.5%) of biomarker–drug pairs for
which PGx testing is required.
9.
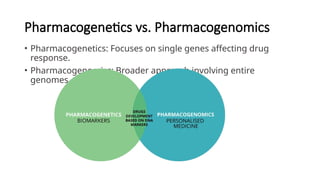
Pharmacogenetics vs. Pharmacogenomics
•Pharmacogenetics: Focuses on single genes affecting drug
response.
• Pharmacogenomics: Broader approach involving entire
genomes.
10.
Pharmacogenetics vs. Pharmacogenomics
•The European Agency for the Evaluation of Medicinal
Products (EMEA) defines “pharmacogenetics” as “the study
of interindividual variations in DNA sequence related to
drug response”
• “pharmacogenomics” as “the study of the variability of the
expression of individual genes relevant to disease
susceptibility as well as drug response at cellular, tissue,
individual or population level” (The European Agency for the
Evaluation of Medicinal Products (EMEA), 2002).
11.
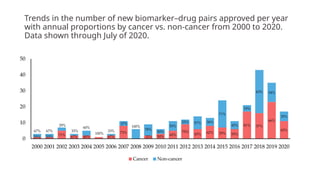
Trends in thenumber of new biomarker–drug pairs approved per year
with annual proportions by cancer vs. non-cancer from 2000 to 2020.
Data shown through July of 2020.
12.
The Pharmacogenomics
Knowledge Base(PharmGKB): A
Vital Resource
The PharmGKB is a
comprehensive
database that provides
information on the
genetic basis of drug
response. It houses a
wealth of data on genes,
drugs, and their
interactions, serving as
a valuable resource for
researchers, clinicians,
and patients.
The PharmGKB allows
users to search for
specific genes, drugs, or
drug-gene interactions.
It provides detailed
information on the
clinical implications of
genetic variations,
helping clinicians make
informed decisions
about drug selection
and dosage.
The PharmGKB also
includes educational
resources and tools to
promote the
understanding and
application of
pharmacogenomics. It
plays a vital role in
advancing personalized
medicine by facilitating
knowledge sharing and
collaboration among
healthcare
professionals.
13.
Enhancing Drug Safetyand
Efficacy: The Role of
Pharmacogenetic Testing
Pharmacogenetic testing can significantly improve drug safety by
identifying patients at risk for adverse reactions. This information
allows doctors to choose alternative medications or adjust dosages
to minimize the risk of complications.
By identifying patients who are likely to respond well to specific
medications, pharmacogenetic testing can enhance drug
efficacy, ensuring that individuals receive the most effective
treatment for their condition.
Pharmacogenetic testing can also help reduce healthcare
costs by minimizing unnecessary hospitalizations, medication
changes, and other complications associated with ineffective
or poorly tolerated medications.
14.
Individual variation
Variability isa serious problem; if not considered, it
can result in:
• Lack of efficacy
• Unexpected harmful effects
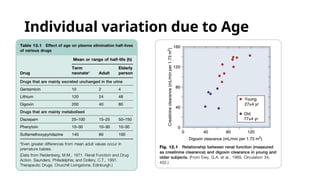
Main causes of variability:
• Age
• Genetic factors
• Immunological factors
• Disease (especially conditions affecting drug
metabolism or elimination, e.g., kidney or liver
disease)
• Drug interactions
15.
• Pharmacokinetic variation:can occur because of differences in
absorption, distribution, metabolism or excretion.
• Pharmacodynamic variation: refers to how individuals respond
differently to drugs. Some drugs, like vaccines and oral contraceptives,
have predictable responses allowing for standard doses. However,
drugs like lithium, antihypertensives, and anticoagulants often require
personalized dosing, adjusted based on plasma drug levels, effects
(e.g., blood pressure changes), and potential side effects.
Individual variation
Key Genes inPharmacogenetic Testing: CYP2D6,
CYP2C9, and CYP2C19
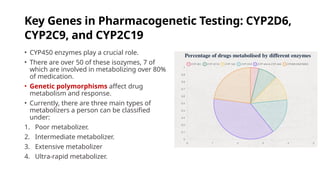
• CYP450 enzymes play a crucial role.
• There are over 50 of these isozymes, 7 of
which are involved in metabolizing over 80%
of medication.
• Genetic polymorphisms affect drug
metabolism and response.
• Currently, there are three main types of
metabolizers a person can be classified
under:
1. Poor metabolizer.
2. Intermediate metabolizer.
3. Extensive metabolizer
4. Ultra-rapid metabolizer.
18.
Key Genes inPharmacogenetic Testing: CYP2D6,
CYP2C9, and CYP2C19
1
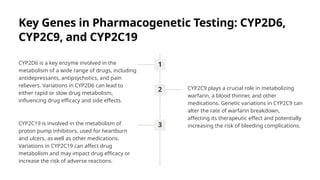
CYP2D6 is a key enzyme involved in the
metabolism of a wide range of drugs, including
antidepressants, antipsychotics, and pain
relievers. Variations in CYP2D6 can lead to
either rapid or slow drug metabolism,
influencing drug efficacy and side effects.
2 CYP2C9 plays a crucial role in metabolizing
warfarin, a blood thinner, and other
medications. Genetic variations in CYP2C9 can
alter the rate of warfarin breakdown,
affecting its therapeutic effect and potentially
increasing the risk of bleeding complications.
3
CYP2C19 is involved in the metabolism of
proton pump inhibitors, used for heartburn
and ulcers, as well as other medications.
Variations in CYP2C19 can affect drug
metabolism and may impact drug efficacy or
increase the risk of adverse reactions.
19.
Individual variation dueto Disease
Therapeutic drugs are prescribed to patients, making the impact of disease on drug
response crucial, especially in conditions affecting major organs responsible for
drug metabolism and excretion.
Diseases Affecting Receptors:
• Myasthenia gravis: Autoimmune disease with antibodies against nicotinic
acetylcholine receptors, leading to increased sensitivity to neuromuscular-blocking
agents (e.g., vecuronium) and aminoglycoside antibiotics.
• X-linked nephrogenic diabetes insipidus: Characterized by abnormal
vasopressin (ADH) receptors, causing insensitivity to ADH.
• Familial hypercholesterolemia: An inherited LDL receptor disorder; homozygous
form resists statin therapy, while the heterozygous form responds well.
20.
Diseases Affecting SignalTransduction:
• Pseudohypoparathyroidism: Results from impaired G protein–
coupled receptor signaling with adenylyl cyclase.
• Familial precocious puberty & hyperthyroidism: Caused by
mutations in G protein–coupled receptors, leading to continuous
receptor activation even without natural hormone stimulation.
Individual variation due to Disease
21.
GENETIC VARIATION
• Mutationsare heritable changes in the DNA base sequence, which
may or may not alter the amino acid sequence of the corresponding
protein.
• Germline or hereditary mutations affect reproductive cells (egg or
sperm) and are passed to the next generation, being present in all
cells of the offspring. (less significant in clinical practice).
• Somatic or acquired mutations are not present at birth but can occur
in any of the body cells (except the ova and sperm) during a lifetime,
and are not passed on to the offspring. (majority not significant in
clinical practice except those involved in cell growth, division, and
differentiation can predispose individuals to carcinogenesis, such
mutations guides drug selection)
22.
PLASMA CHOLINESTERASE DEFICIENCY
•Suxamethonium sensitivity is due to genetic variation in the rate of
drug metabolism, resulting from a Mendelian autosomal recessive trait.
This short-acting neuromuscular-blocking drug is widely used in
anesthesia and is normally rapidly hydrolyzed by plasma cholinesterase.
• About 1 in 3,000 individuals fail to inactivate Suxamethonium rapidly
and experience prolonged neuromuscular block when treated with it.
This occurs because a recessive gene produces an abnormal type of
plasma cholinesterase.
• The abnormal enzyme has a modified pattern of substrate and inhibitor
specificity. It can be detected by a blood test that measures the effect of
dibucaine, which inhibits the abnormal enzyme less effectively than the
normal enzyme.
23.
PLASMA CHOLINESTERASE DEFICIENCY
•They appear completely healthy unless exposed to
suxamethonium or mivacurium (which is also inactivated by
plasma cholinesterase), but experience prolonged paralysis if
exposed to a dose that would cause neuromuscular block for
only a few minutes in a healthy person.
• It is important to check the family history and test family
members who may be affected. However, the disorder is so rare
that it is currently impractical to screen for it routinely before the
therapeutic use of suxamethonium.
24.
Integrating Pharmacogenetics into
Clinicalapplications.
• Clinical tests to predict drug responsiveness were among the
earliest anticipated applications of human genome sequencing.
• New pharmacogenetic tests must demonstrate a positive or
meaningful impact on prescribing practices, such as guiding the
selection of an alternative drug or adjusting the dosing regimen
to achieve measurable improvements in patient outcomes
(Khoury & Galea, 2016).
25.
Integrating Pharmacogenetics into
Clinicalapplications.
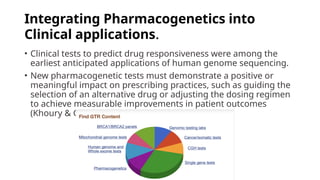
• Pharmacogenetic evaluation can include tests for:
• HLA Variants – Associated with severe drug reactions
due to immunological interactions.
• Human leukocyte antigen (HLA) system is a complex
of genes on chromosome 6 in humans that encode cell-
surface proteins responsible for regulation of
the immune system.
• Genes controlling aspects of drug metabolism.
• Genes encoding drug targets, where FDA defines them
as tests guiding drug selection based on
pharmacogenetic markers (Ko et al., 2015)
26.
Integrating Pharmacogenetics into
Clinicalapplications.
• Pharmacogenetics are incorporated into daily clinical workflows and
the main area of Application are:
• INDICATIONS: where genetic information helps us decide whether the
particular drug is indicated, or not.
• Dosage adjustment based on genetic predictors of drug metabolism:
highlight two prominent examples where dosing schedule is can be
guided by evaluation of genetic variants.
• Screening out patients who are highly susceptible to serious adverse
drug reactions.
• Communicating the presence or absence of risk.
27.
Pharmacogenetics in Clinicalapplications:
indication
• Trastuzumab (Herceptin) is a
monoclonal antibody that
antagonises epidermal growth
factor (EGF) by binding to one of its
receptors (human EGF receptor 2 -
HER2) which can occur in tumour
tissue as a result of somatic
mutation. It is used in patients with
breast cancer whose tumour tissue
is positive for this receptor.
28.
Pharmacogenetics in Clinicalapplications:
indication
• Dasatinib and imatinib are first-line tyrosine
kinase inhibitors used in haematological
malignancies characterised by the presence of a
Philadelphia chromosome, namely chronic
myeloid leukaemia (CML) and in some adults with
acute lymphocytic leukaemia (ALL).
• The Philadelphia chromosome results from a
translocation defect when parts of two
chromosomes (9 and 22) swap places; part of a
'breakpoint cluster region' (BCR) in chromosome
22 links to the 'Abelson-1' (ABL) region of
chromosome 9.
29.
Pharmacogenetics in Clinicalapplications:
indication
• A mutation (T3151) in BCR/ABL confers
resistance to the inhibitory effect of
dasatinib and patients with this variant
do not benefit from this drug.
• Instead, ponatinib is licensed in the
United States for treatment of patients
who have this BCR-ABL T3151 mutation.
30.
Pharmacogenetics in Clinicalapplications:
indication
• There are now small-molecule-based treatments specifically
targeted at patients with certain defined inherited conditions.
• These include:
• Givosiran (GIVLAARI) indicated for the treatment of adults
with acute hepatic porphyria (AHP).
• Eteplersen (Exondys-51): an antisense oligomer that acts on
mRNA to restore dystrophin production, for patients with
highly specific mutations that cause Duchenne/Becker
muscular dystrophy (DMD).
• The recommended dose of GIVLAARI is 2.5 mg/kg
administered via subcutaneous injection once monthly
by HCPs.
31.
Pharmacogenetics in Clinicalapplications:
dosage adjustment
Thiopurine Drugs:
• Tioguanine, Mercaptopurine, and Azathioprine are used for
leukemias and immunosuppression in inflammatory disorders (bowel,
skin, joints).
• These drugs are detoxified by thiopurine-S-methyltransferase (TPMT)
and xanthine oxidase.
• Genetic variants in TPMT affect drug metabolism.
• Reduced doses recommended for patients with low TPMT activity.
• Genetic testing helps but does not eliminate toxicity risks.
• White blood cell count must be closely monitored, as environmental
factors also impact toxicity. (Weinshilboum and Sladek, 1980).
32.
Pharmacogenetics of 5-FUand Related Drugs
5-Fluorouracil (5-FU), Capecitabine, Tegafur
• Used for solid tumors but have a narrow therapeutic window.
• Toxicity Risks:
• 10%-40% of patients experience severe side effects (neutropenia, vomiting,
diarrhea, mucocutaneous syndromes).
• Fatality rate: ~1 in 100.
• 80% of 5-FU is detoxified by dihydropyrimidine dehydrogenase (DPYD).
• Four major DPYD variants contribute to 20%-30% of life-threatening toxicity
cases.
Clinical Application:
• Genetic testing guides dose reductions and gradual dose increments.
• May help select alternative chemotherapy for high-risk patients.
33.
Pharmacogenetics in Clinicalapplications:
Screening
Abacavir (HIV Treatment)
• Reverse transcriptase inhibitor effective for
HIV.
• Its use has been limited by severe rashes.
Susceptibility to this adverse effect is closely
linked to the HLA variant HLAB*5701.
• Genetic testing is now standard of care to
prevent hypersensitivity reactions. (Martin
and Kroetz, 2013).
34.
Pharmacogenetics in Clinicalapplications:
Screening
Carbamazepine and HLA-B*1502 Screening
• Carbamazepine can cause severe Skin Reactions such as:
• Stevens-Johnson Syndrome (SJS) & Toxic Epidermal Necrolysis (TEN).
• Characterized by painful blistering, skin detachment, and potential
gastrointestinal involvement.
• Strongly linked to HLA-B*1502 allele.
• More common in Thailand, Malaysia, and Taiwan.
• Less frequent in Korean, Japanese, and White populations.
• HLA-B*1502 screening prevents carbamazepine-induced SJS
(Barbarinoet al., 2015).
35.
Pharmacogenetics in Clinicalapplications:
Communicating the presence or absence of risk
• a particular drug may have been specifically tested in people with
different genetic variants, and there may be information on extent of
risk, if any.
• lacosamide (used in the treatment of epilepsy): no clinically relevant
difference in lacosamide exposure when comparing extensive
metabolizers against poor metabolizers according to CYP2C19 status
36.
The Future ofMedicine:
Integrating
Pharmacogenetics into
Clinical Practice
The future of medicine holds great promise for
personalized therapy as pharmacogenetics becomes
increasingly integrated into clinical practice.
The ongoing advancements in genomic sequencing,
bioinformatics, and drug development will further
refine and expand the applications of
pharmacogenetics, leading to more effective and
safer treatments for a wide range of conditions.
This paradigm shift in healthcare will empower
patients and clinicians to work together, leveraging
the power of individual genetic information to
optimize health outcomes.
37.
References
• Rang, H.P., Dale, M. M., Ritter, J. M., Flower, R. J., & Henderson, G. (2023). Rang & Dale's Pharmacology. 10th ed. Elsevier.
• PharmGKB. (2024). Pharmacogenomics Knowledge Base. Available at: https://www.pharmgkb.org/ [Accessed 24 Feb 2025].
• FDA. (2025). Table of Pharmacogenetic Biomarkers in Drug Labeling. Available at: https://www.fda.gov/[Accessed 24 Feb 2025].
• Barbarino, J.M., Kroetz, D.L., Klein, T.E., Altman, R.B., 2015. PharmGKB Summary: Very Important Pharmacogene Information for Human Leukocyte
Antigen B (HLA-B). Pharmacogenet. Genomics 25, 205–221. https://doi.org/10.1097/FPC.0000000000000118
• Gonzales, A., Collantes-Silva, N., Arambulo-Castillo, S., Ortiz-Benique, Z.N., Alarcon, E., 2024. Abstract 4140060: Impact of SGLT2 Inhibitors on Mortality
Risk in Type 2 Diabetes Mellitus and Coronary Artery Disease: A Systematic Review and Meta-Analysis. Circulation 150.
https://doi.org/10.1161/circ.150.suppl_1.4140060
• Khoury, M.J., Galea, S., 2016. Will Precision Medicine Improve Population Health? JAMA 316, 1357–1358. https://doi.org/10.1001/jama.2016.12260
• Ko, T.-M., Tsai, C.-Y., Chen, S.-Y., Chen, K.-S., Yu, K.-H., Chu, C.-S., Huang, C.-M., Wang, C.-R., Weng, C.-T., Yu, C.-L., Hsieh, S.-C., Tsai, J.-C., Lai, W.-T., Tsai, W.-
C., Yin, G.-D., Ou, T.-T., Cheng, K.-H., Yen, J.-H., Liou, T.-L., Lin, T.-H., Chen, D.-Y., Hsiao, P.-J., Weng, M.-Y., Chen, Y.-M., Chen, Chen-Hung, Liu, M.-F., Yen, H.-
W., Lee, J.-J., Kuo, M.-C., Wu, C.-C., Hung, S.-Y., Luo, S.-F., Yang, Y.-H., Chuang, H.-P., Chou, Y.-C., Liao, H.-T., Wang, C.-W., Huang, C.-L., Chang, C.-S., Lee, M.-
T.M., Chen, P., Wong, C.-S., Chen, Chien-Hsiun, Wu, J.-Y., Chen, Y.-T., Shen, C.-Y., Taiwan Allopurinol-SCAR Consortium, 2015. Use of HLA-B*58:01
genotyping to prevent allopurinol induced severe cutaneous adverse reactions in Taiwan: national prospective cohort study. BMJ 351, h4848.
https://doi.org/10.1136/bmj.h4848
• Martin, M.A., Kroetz, D.L., 2013. Abacavir Pharmacogenetics – From Initial Reports to Standard of Care. Pharmacotherapy 33, 765–775.
https://doi.org/10.1002/phar.1278
• Pian, P.M.T., Galinkin, J.L., Davis, P.J., 2017. 11 - Opioids, in: Davis, P.J., Cladis, F.P. (Eds.), Smith’s Anesthesia for Infants and Children (Ninth Edition).
Elsevier, Philadelphia, pp. 219-238.e7. https://doi.org/10.1016/B978-0-323-34125-7.00011-5
• Weinshilboum, R.M., Sladek, S.L., 1980. Mercaptopurine pharmacogenetics: Monogenic inheritance of erythrocyte thiopurine methyltransferase activity.
Am. J. Hum. Genet. 32, 651.




![References
• Rang, H. P., Dale, M. M., Ritter, J. M., Flower, R. J., & Henderson, G. (2023). Rang & Dale's Pharmacology. 10th ed. Elsevier.
• PharmGKB. (2024). Pharmacogenomics Knowledge Base. Available at: https://www.pharmgkb.org/ [Accessed 24 Feb 2025].
• FDA. (2025). Table of Pharmacogenetic Biomarkers in Drug Labeling. Available at: https://www.fda.gov/[Accessed 24 Feb 2025].
• Barbarino, J.M., Kroetz, D.L., Klein, T.E., Altman, R.B., 2015. PharmGKB Summary: Very Important Pharmacogene Information for Human Leukocyte
Antigen B (HLA-B). Pharmacogenet. Genomics 25, 205–221. https://doi.org/10.1097/FPC.0000000000000118
• Gonzales, A., Collantes-Silva, N., Arambulo-Castillo, S., Ortiz-Benique, Z.N., Alarcon, E., 2024. Abstract 4140060: Impact of SGLT2 Inhibitors on Mortality
Risk in Type 2 Diabetes Mellitus and Coronary Artery Disease: A Systematic Review and Meta-Analysis. Circulation 150.
https://doi.org/10.1161/circ.150.suppl_1.4140060
• Khoury, M.J., Galea, S., 2016. Will Precision Medicine Improve Population Health? JAMA 316, 1357–1358. https://doi.org/10.1001/jama.2016.12260
• Ko, T.-M., Tsai, C.-Y., Chen, S.-Y., Chen, K.-S., Yu, K.-H., Chu, C.-S., Huang, C.-M., Wang, C.-R., Weng, C.-T., Yu, C.-L., Hsieh, S.-C., Tsai, J.-C., Lai, W.-T., Tsai, W.-
C., Yin, G.-D., Ou, T.-T., Cheng, K.-H., Yen, J.-H., Liou, T.-L., Lin, T.-H., Chen, D.-Y., Hsiao, P.-J., Weng, M.-Y., Chen, Y.-M., Chen, Chen-Hung, Liu, M.-F., Yen, H.-
W., Lee, J.-J., Kuo, M.-C., Wu, C.-C., Hung, S.-Y., Luo, S.-F., Yang, Y.-H., Chuang, H.-P., Chou, Y.-C., Liao, H.-T., Wang, C.-W., Huang, C.-L., Chang, C.-S., Lee, M.-
T.M., Chen, P., Wong, C.-S., Chen, Chien-Hsiun, Wu, J.-Y., Chen, Y.-T., Shen, C.-Y., Taiwan Allopurinol-SCAR Consortium, 2015. Use of HLA-B*58:01
genotyping to prevent allopurinol induced severe cutaneous adverse reactions in Taiwan: national prospective cohort study. BMJ 351, h4848.
https://doi.org/10.1136/bmj.h4848
• Martin, M.A., Kroetz, D.L., 2013. Abacavir Pharmacogenetics – From Initial Reports to Standard of Care. Pharmacotherapy 33, 765–775.
https://doi.org/10.1002/phar.1278
• Pian, P.M.T., Galinkin, J.L., Davis, P.J., 2017. 11 - Opioids, in: Davis, P.J., Cladis, F.P. (Eds.), Smith’s Anesthesia for Infants and Children (Ninth Edition).
Elsevier, Philadelphia, pp. 219-238.e7. https://doi.org/10.1016/B978-0-323-34125-7.00011-5
• Weinshilboum, R.M., Sladek, S.L., 1980. Mercaptopurine pharmacogenetics: Monogenic inheritance of erythrocyte thiopurine methyltransferase activity.
Am. J. Hum. Genet. 32, 651.](https://image.slidesharecdn.com/pharmacogenomics-250312100353-d2fd92cf/85/pharmacogenomics-and-personalized-therapy-pptx-37-320.jpg)











































![The-Case-for-Practice-Integration[1]](https://cdn.slidesharecdn.com/ss_thumbnails/f8309d43-8226-4580-ab57-0beb0b770357-160412231650-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








