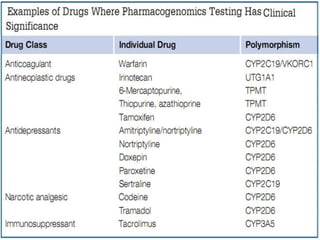
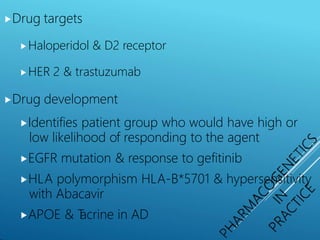
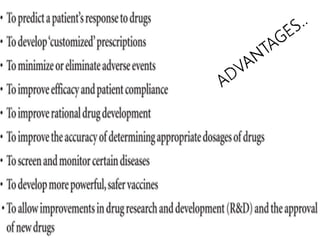
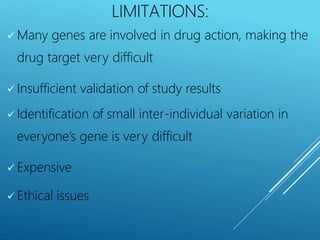
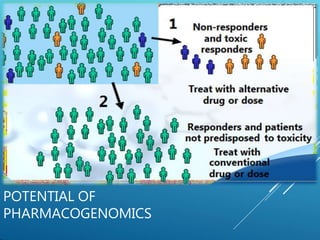
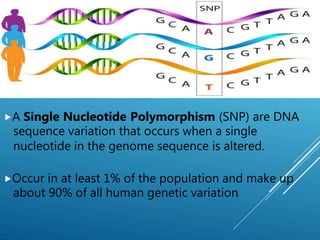
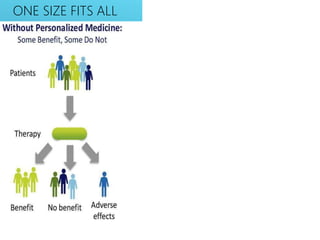
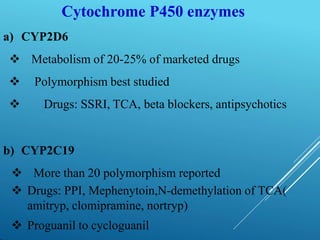
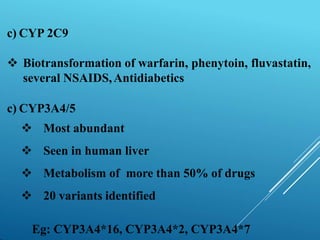
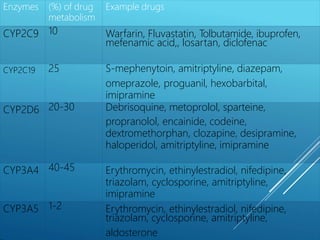
This document provides an outline and overview of pharmacogenomics. It begins by defining pharmacogenomics as the study of how genetic inheritance affects drug response. It describes how variants such as mutations and single nucleotide polymorphisms (SNPs) can influence drug metabolism and efficacy. The document outlines several examples of polymorphisms in important drug-metabolizing enzymes like cytochrome P450 and how this can impact drug levels. It also discusses the potential for pharmacogenomics to enable personalized medicine by identifying genetic factors that make individuals more or less likely to respond to certain drugs. However, it notes there are also limitations to pharmacogenomics in terms of cost, validation challenges, and difficulty given multiple genetic factors can influence drug actions.



![⯈Insulin resistance
⯈ Polygenic[ Ark-I, Atl, Minn]
⯈ Insulin receptor α subunit
⯈Arrhythmia with antiarrhythmics
⯈ T
orsades de pointes
⯈ Genetic abnormality in k+ channel(polymorphism)
⯈Resistance to drug effects
⯈ Vit D resistance rickets
⯈ Coumarin resistance( polymorphism of vit K reductase)](https://image.slidesharecdn.com/pharmacogenomics-171011132627-230117110318-8309ff28/85/pharmacogenomics-171011132627-pptx-25-320.jpg)