Downloaded 1,411 times

















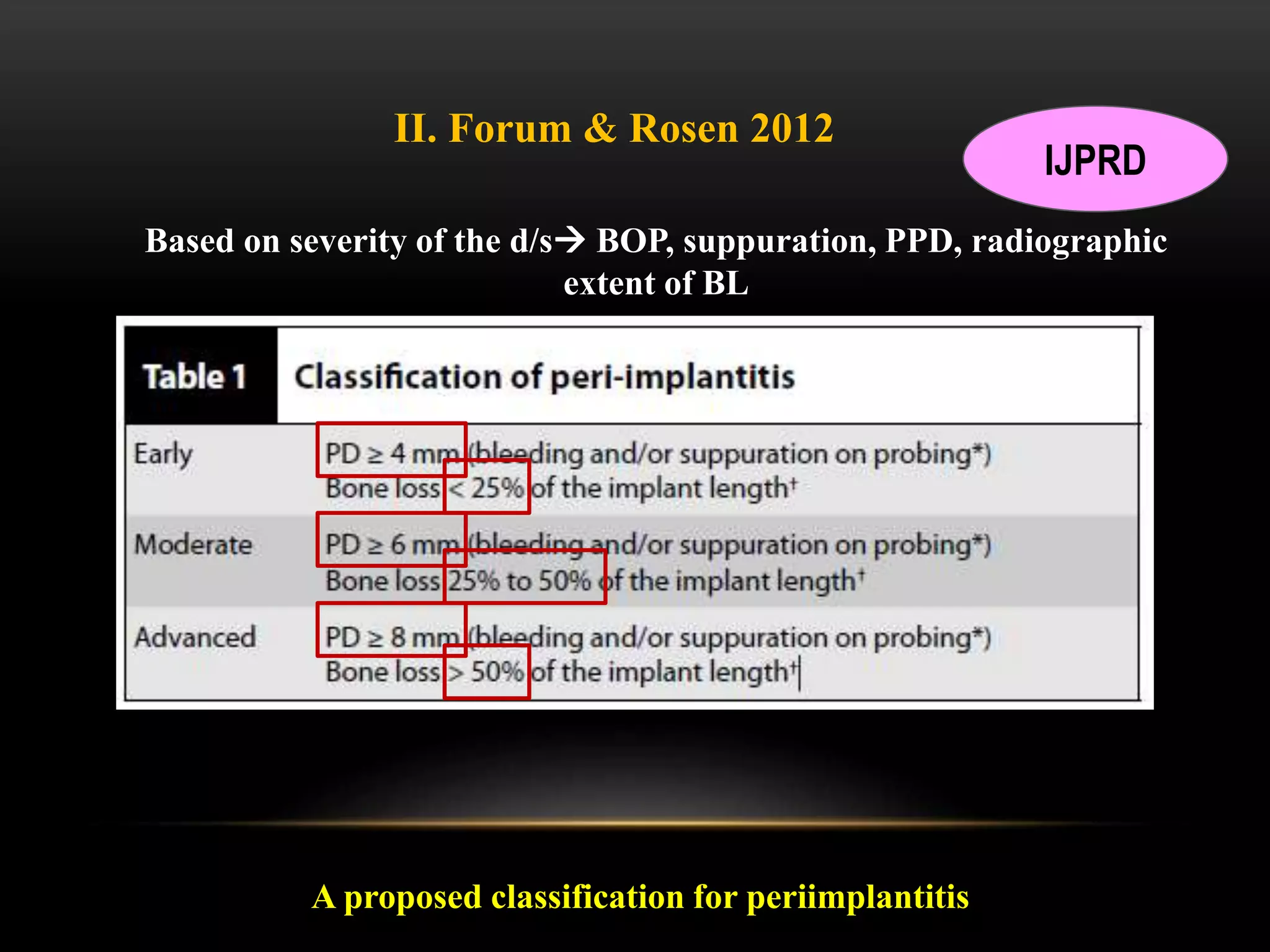







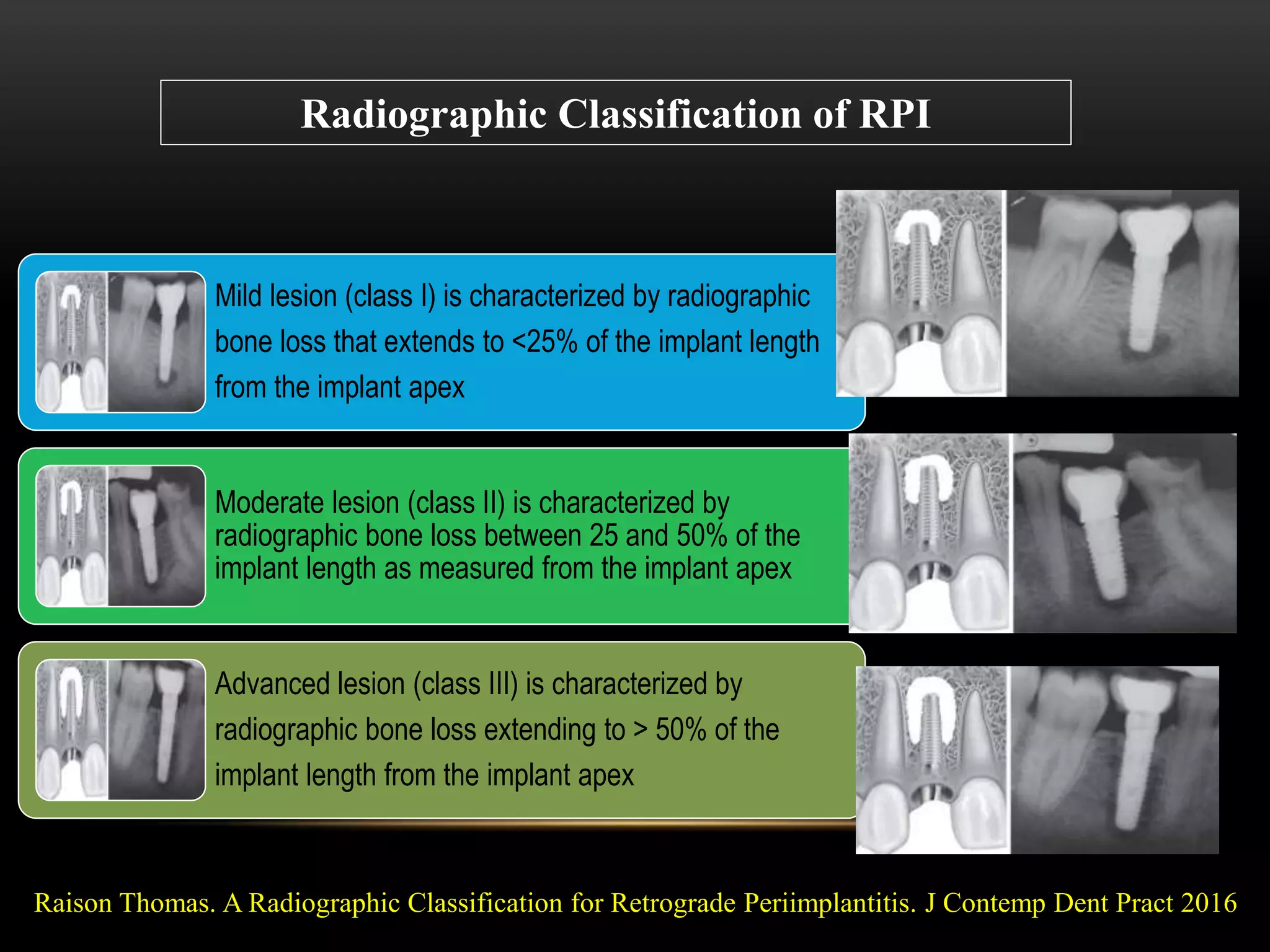















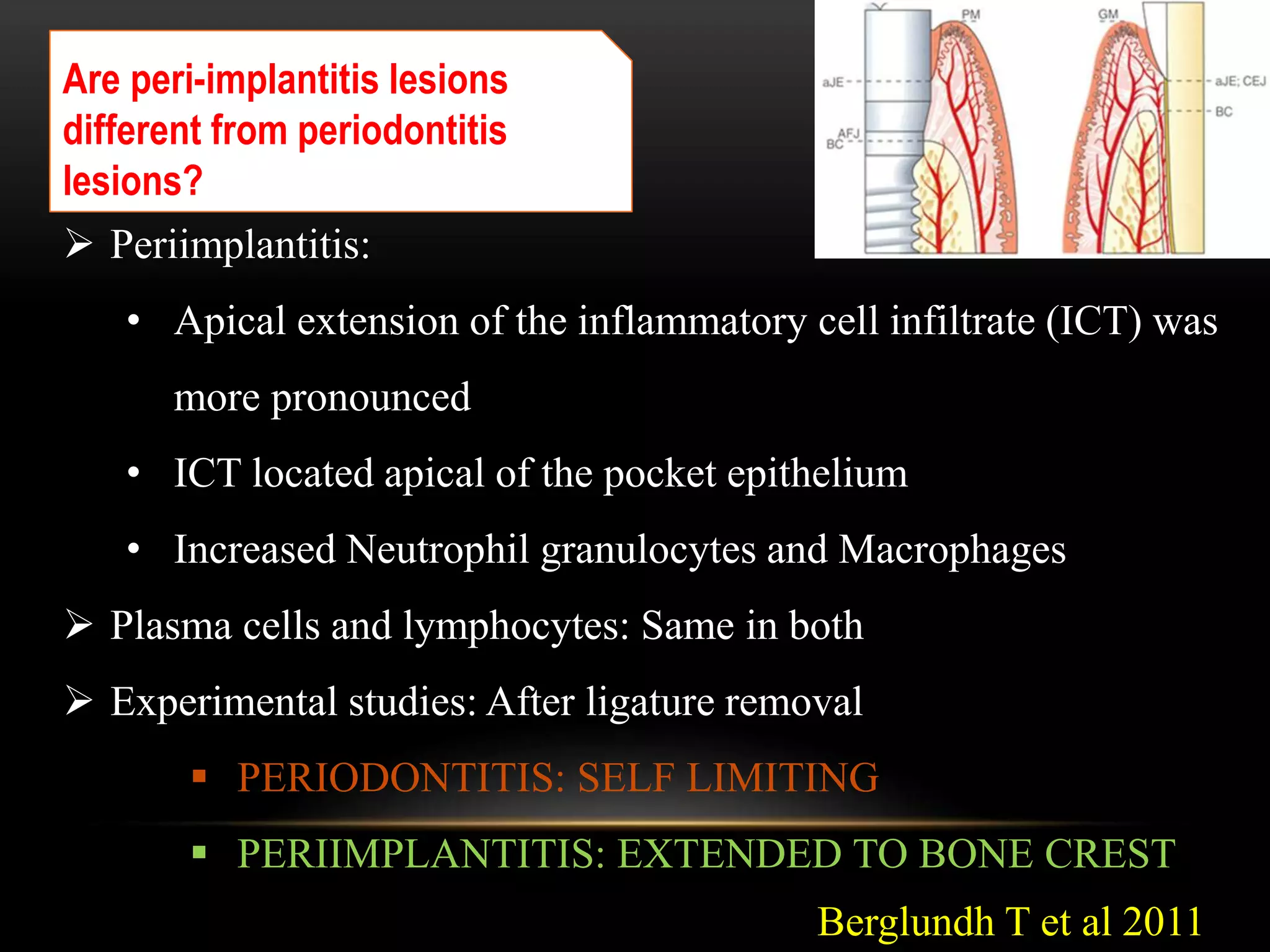












































This document provides an overview of periimplantitis, including its definition, classification systems, epidemiology, etiology, pathogenesis, diagnosis, and treatment. Periimplantitis is defined as an inflammatory process involving both soft and hard tissues around a dental implant, resulting in loss of supporting bone. It is distinguished from peri-implant mucositis, which only involves inflammation of soft tissues. The document discusses various classification systems for periimplantitis and reviews potential etiologic factors such as plaque, biomechanical overload, genetic factors, and iatrogenic causes. Diagnosis involves clinical parameters like bleeding, probing depth, and radiographic bone loss. Treatment aims to eliminate infection and may include nonsurgical and surgical











































































































