Dental implant andimplant failures
■ Dental implant (also known as an endosseous implant or fixture) is a prosthesis that
interfaces with the bone of the jaw or skull to support a dental prosthesis such as a
crown, bridge, denture, or facial prosthesis or to act as an orthodontic anchor.
■ Implant failure causes :
■ Early - Overheating, contamination and trauma during surgery, poor bone quantity
and/or quality, lack of primary stability, and incorrect immediate load indication
■ Late - Periimplantitis, occlusal trauma, and overloading
A dental implant is considered to be a failure if it is lost, mobile, or shows peri-implant
bone loss of greater than 1.0 mm in the first year
5.
Differences between...
Peri-implant
mucosa
■ Directbone-to-implant contact
■ Subepithelially more collagen fibers
and less fibroblasts/vessels
■ Parallel collagen fibers in relation
to implant surface
Physiological
periodontium
■ Anchoring system of root
cementum, alveolar bone and
desmodontic fibers
■ Subepithelially more fibroblasts
and vessels
■ Dentogingival, dentoperiostal,
circular and transseptal fiber
orientation
6.
Desmosomes and hemidesmosomesof epithelium and
junctional epithelium (biological width) are linked with the
contact surface
7.
Etiology
• Multi factorial,poly-microbial anaerobic infection
• Microbial biofilm: Prevotella intermedia, Prevotella nigrescens, Streptococcus constellatus,
Aggregatibacter actinomycetemcomitans, Porphyromonas gingivalis, Treponema
denticola and Tannerella forsythia
• Staphylococcus aureus appears to play a predominant role for the development of a peri-
implantitis, according to the results of Salvi et al This bacterium shows a high affinity to titanium.
• Smoking
• History of periodontitis.
• Lack of compliance and limited oral hygiene (including missing checkups).
Systemic diseases (e.g. maladjusted diabetes mellitus, cardiovascular disease,
immunosuppression) and drug therapies, which inhibit bone modulations
• Iatrogenic causes (FBR)
• Soft tissue defects or poor-quality soft tissue at the area of implantation (e.g. lack of keratinized
gingiva).
• History of one or more failures of implants
In a study by Ver vaeke et al. maxillary implants were at a significantly higher risk for peri-implant
bone loss compared to mandibular implants
8.
Pathogenesis
Formation of salivarypellicle consisting of salivary proteins and peptides
Initiation of bacterial colonization
The high-molecular-weight mucins, salivary α-amylase, and proline-rich glycoproteins.(salivary
pellicles on titanium )
nonmotile coccoid cells and gram negative spirochetes
mediates microorganisms’ adhesion.
Cement and titanium particles take part in the breakdown of the established equilibrium.
• As a response to this triggering factor,(FBR) complement and macrophages become activated
and upregulate osteoclastic activities leading to marginal bone loss.
Peri-implant bony lesions usually follow a typical crater shape rather than the atypical periodontal
bone loss.
9.
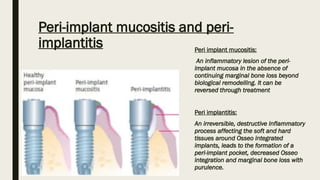
Peri-implant mucositis andperi-
implantitis Peri implant mucositis:
An inflammatory lesion of the peri-
implant mucosa in the absence of
continuing marginal bone loss beyond
biological remodelling. It can be
reversed through treatment
Peri implantitis:
An irreversible, destructive Inflammatory
process affecting the soft and hard
tissues around Osseo integrated
implants, leads to the formation of a
peri-implant pocket, decreased Osseo
integration and marginal bone loss with
purulence.
11.
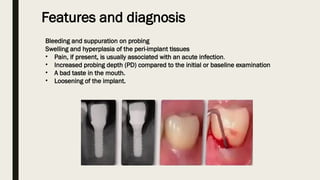
Features and diagnosis
Bleedingand suppuration on probing
Swelling and hyperplasia of the peri-implant tissues
• Pain, if present, is usually associated with an acute infection.
• Increased probing depth (PD) compared to the initial or baseline examination
• A bad taste in the mouth.
• Loosening of the implant.
12.
1. Biomarkers inperi-implant crevicular fluid (PICF)[proinflammatory cytokines (IL-1β, TNFα, MMP-
8) ] and GCF (MMP-8, MMP-9, Osteoprotegerin, C-reactive Protein and IL-1β) show promising
results in regard to their diagnostic and prognostic value.
2. Since RANKL and OPG are key factors regulating bone metabolism, it is likely they are involved
in alveolar bone destruction in PI
3. Metabolomic analysis, mass spectrometry and nuclear magnetic resonance spectroscopy show
promise.
• In the absence of initial radiographs and probing depths, radiographic evidence of bone loss of ≥3
mm and/or probing depths ≥6 mm in conjunction with profuse bleeding fits the definition for PI.
• Radiographically a typical crater shape rather than the atypical periodontal bone loss is seen
cervically.
• Apical portion is still osseointegrated








![1. Biomarkers in peri-implant crevicular fluid (PICF)[proinflammatory cytokines (IL-1β, TNFα, MMP-
8) ] and GCF (MMP-8, MMP-9, Osteoprotegerin, C-reactive Protein and IL-1β) show promising
results in regard to their diagnostic and prognostic value.
2. Since RANKL and OPG are key factors regulating bone metabolism, it is likely they are involved
in alveolar bone destruction in PI
3. Metabolomic analysis, mass spectrometry and nuclear magnetic resonance spectroscopy show
promise.
• In the absence of initial radiographs and probing depths, radiographic evidence of bone loss of ≥3
mm and/or probing depths ≥6 mm in conjunction with profuse bleeding fits the definition for PI.
• Radiographically a typical crater shape rather than the atypical periodontal bone loss is seen
cervically.
• Apical portion is still osseointegrated](https://image.slidesharecdn.com/76periimplantitis-250312151602-5a10dc11/85/periimplantitis-pptx-12-320.jpg)






















































