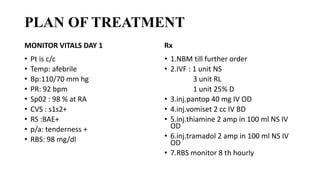
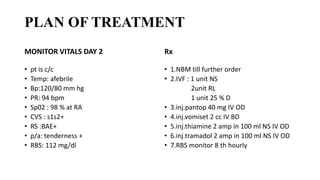
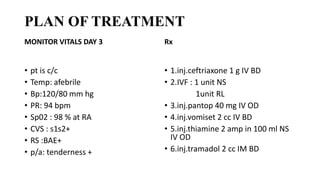
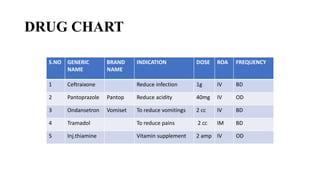


1. A 35-year-old male was admitted to the hospital with abdominal pain and nausea and was diagnosed with acute pancreatitis based on elevated serum amylase and lipase levels and abdominal ultrasound findings. 2. He was treated with IV fluids, pantoprazole, ondansetron, tramadol, thiamine injections, and later ceftriaxone injections. His condition was monitored over three days and showed improvement. 3. Acute pancreatitis can be caused by gallstones, heavy alcohol use, certain medications, and other factors. It leads to inflammation of the pancreas and pain in the upper abdomen. Treatment focuses on pain relief, rehydration, and addressing the























































































