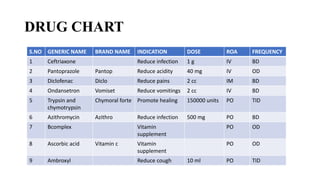


A 35-year-old male presented with a left inguinal hernia. Examination and imaging confirmed a left inguinal hernia with omental fat as the content. The patient underwent a left hernioplasty surgery under spinal anesthesia. Post-operatively, the patient was treated with antibiotics and analgesics. By post-operative day 3, the patient had no complaints and was discharged on medications including antibiotics and supplements.























































































