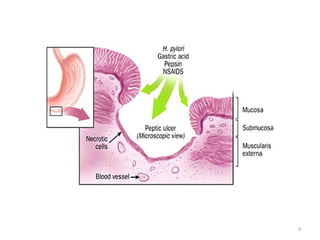
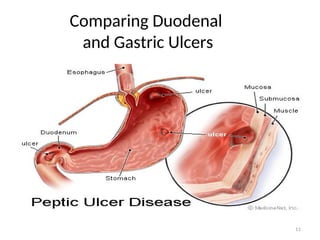
The document provides a comprehensive overview of peptic ulcer disease (PUD), including its definitions, etiology, demographics, diagnosis, and treatment methods. It highlights the roles of Helicobacter pylori and the impact of lifestyle factors such as NSAID use, smoking, and alcohol on ulcer development. Additionally, it discusses complications related to PUD and outlines preventive measures and treatment protocols for both H. pylori-positive and negative cases.




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








