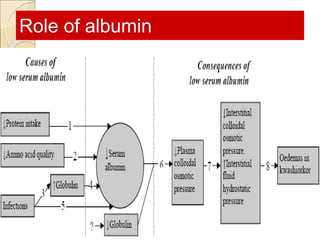
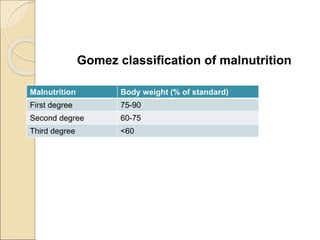
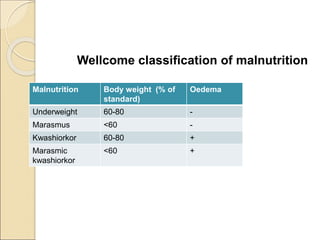
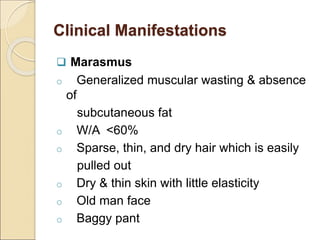
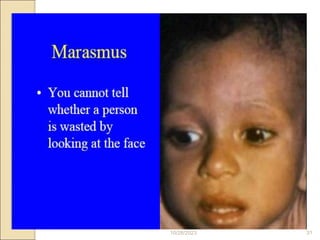
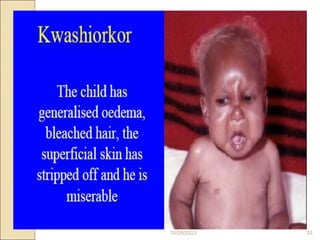
This document discusses pediatric nutrition and malnutrition. It begins by outlining the changing nutritional needs of children based on their age and development. It then discusses the global burden of child malnutrition. The document covers nutritional recommendations for infants from birth to 1 year old, including the benefits of breastfeeding. It also discusses protein-energy malnutrition, providing classifications and clinical manifestations such as marasmus and kwashiorkor. The principles of management are outlined, including resolving life-threatening conditions, restoring nutritional status through feeding phases, and ensuring rehabilitation.










































































![Acid base titration III [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/acidbasetitrationiiicompatibilitymode-231030064045-e32b2458-thumbnail.jpg?width=640&height=640&fit=bounds)









![74676371-Coagulation-and-Flocculation[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/74676371-coagulation-and-flocculation1-260116154109-a3cbf55e-thumbnail.jpg?width=640&height=640&fit=bounds)














