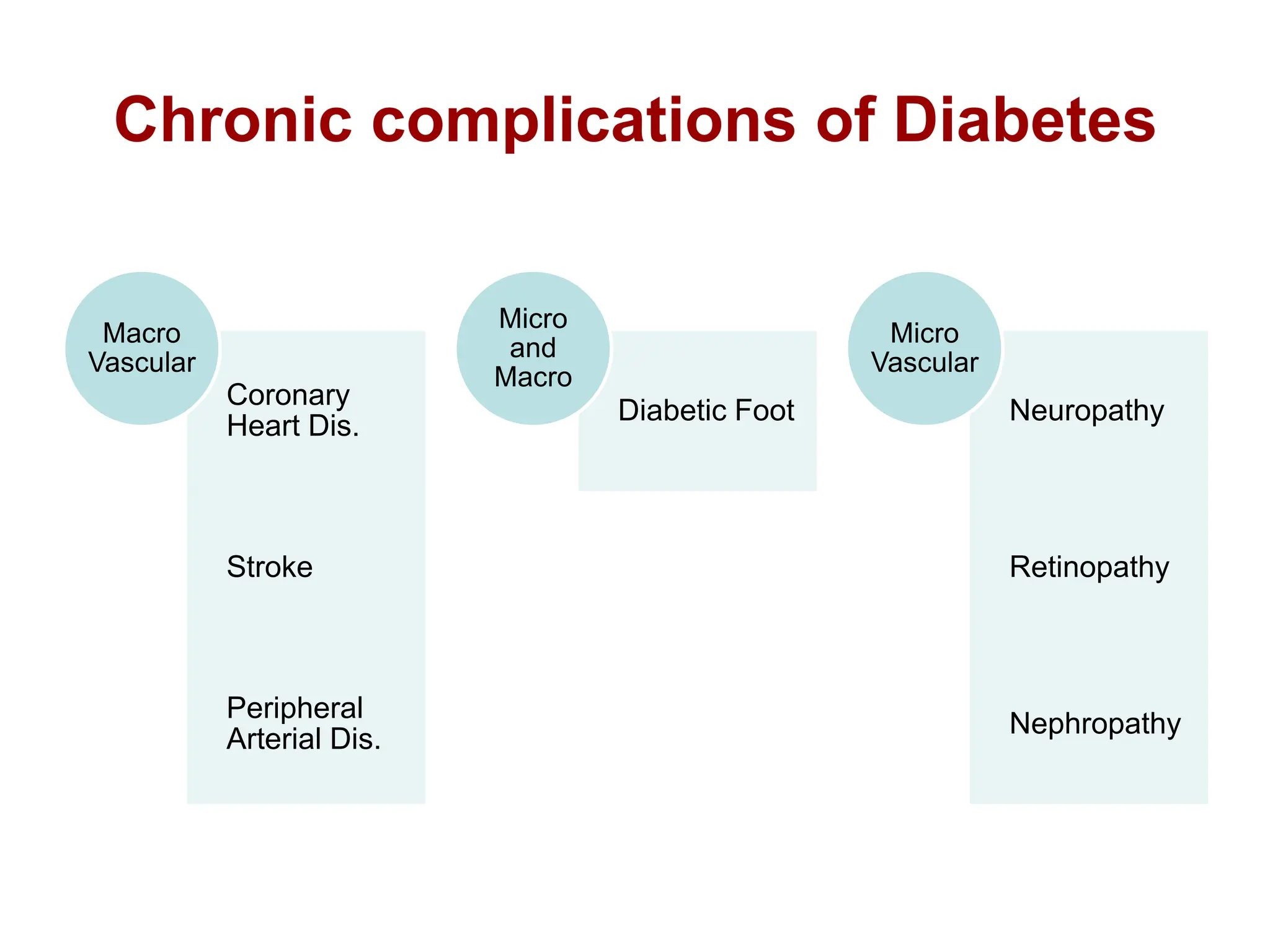
This document summarizes chronic complications of diabetes mellitus, including macrovascular complications like coronary heart disease, stroke, and peripheral arterial disease, as well as microvascular complications like diabetic neuropathy, retinopathy, and nephropathy. It provides details on the pathogenesis, clinical presentation, diagnosis and management of peripheral diabetic neuropathy, noting that tight glycemic control through intensive insulin therapy can help prevent or delay the risk of developing diabetic complications.


































































































































![Acid base titration III [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/acidbasetitrationiiicompatibilitymode-231030064045-e32b2458-thumbnail.jpg?width=640&height=640&fit=bounds)



































