Downloaded 148 times





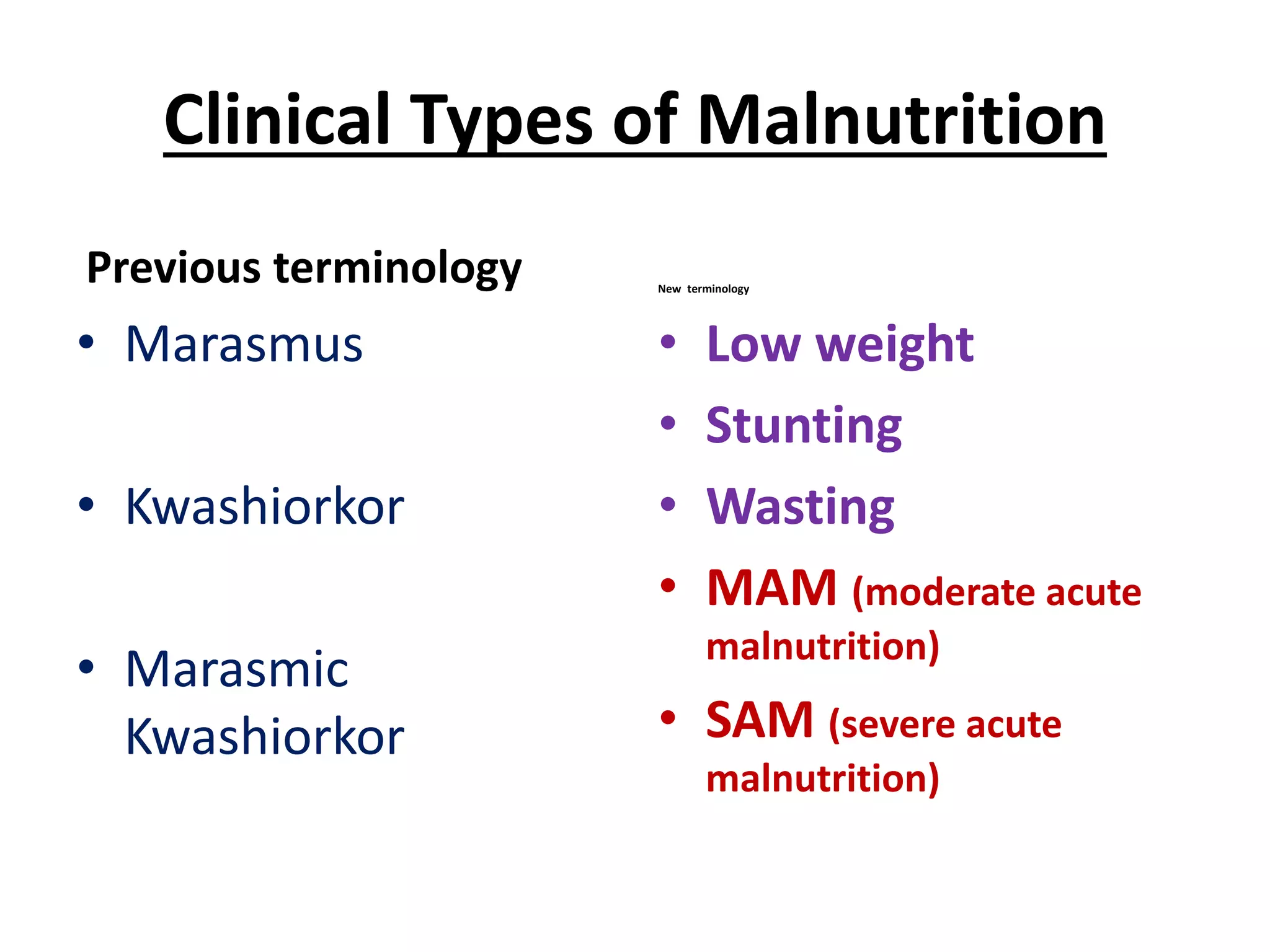



























































































This document discusses malnutrition in children in Pakistan. It provides statistics showing high rates of under-five mortality, infant mortality, and neonatal mortality. The top causes of death in children under 5 are prematurity, pneumonia, and diarrhea. Malnutrition is a major contributing factor to under-five mortality. The document then discusses the high prevalence of malnutrition in Pakistan, including stunting affecting 41% of children, wasting 14%, and underweight affecting 31%. It also notes high rates of micronutrient deficiencies. The main causes of malnutrition are identified as inadequate feeding practices, repeated infections, and poverty. The document concludes with descriptions of different types of malnutrition and their clinical management.























































































